In cooperation with the Orcas Island Health Care District,
Madrona Voices presents the
September 2018 Health Care Survey Report
Written by Steve Smith and Jennifer Smith, Madrona Voices.

For easier navigation, note the Table of Contents. It will allow you to quickly navigate the document. You can return to the Table of Contents by clicking on the small black or orange icon that you will find in the lower right of your screen. You will only see this after you have scrolled down a way on the page.  You can also toggle the Table of Contents by clicking the square to the right of the title, “Table of Contents”.
You can also toggle the Table of Contents by clicking the square to the right of the title, “Table of Contents”. ![]()
Table of Contents
Introduction
The survey design was a collaborative effort between the Orcas Island Health Care District (OIHCD) and Madrona Voices. The survey was released on September 10, 2018. The data for this report was collected for one week, through Sunday, September 16th. The survey was, then, extended through Thursday, September 27th. The added eleven days yielded an additional 39 responses.
This report can be found online at https://www.madronavoices.com/ and may be available on the OIPHCD site https://orcashealth.org/
The survey was sent to our email list. We estimate that this list includes more than half of the email addresses for Orcas Island. We provide a detailed explanation on our website ( madronavoices.com ) about why the results are representative of the community, the methods we use to obtain the results, how we analyze the information, and our commitment to privacy. We do not share or sell any of the personal information, nor do we share who made any of the comments in the survey.
This survey took most people, on average, ten minutes to complete. Those who didn’t add any comments could complete the survey in about five minutes. Those who added comments often took longer. A person could complete the survey and re-enter it in order to modify their answers or comments.
This survey packed a lot of information into a small space. The matrix questions, where we presented options in both rows and columns, allowed the participant to quickly respond. But, for reporting purposes, each row is a separate concept. The typical participant saw:
- 15 multiple-choice questions, 5 of which were demographic in nature.
- 4 matrix questions where 14 separate concepts were asked about.
- 6 comment opportunities.
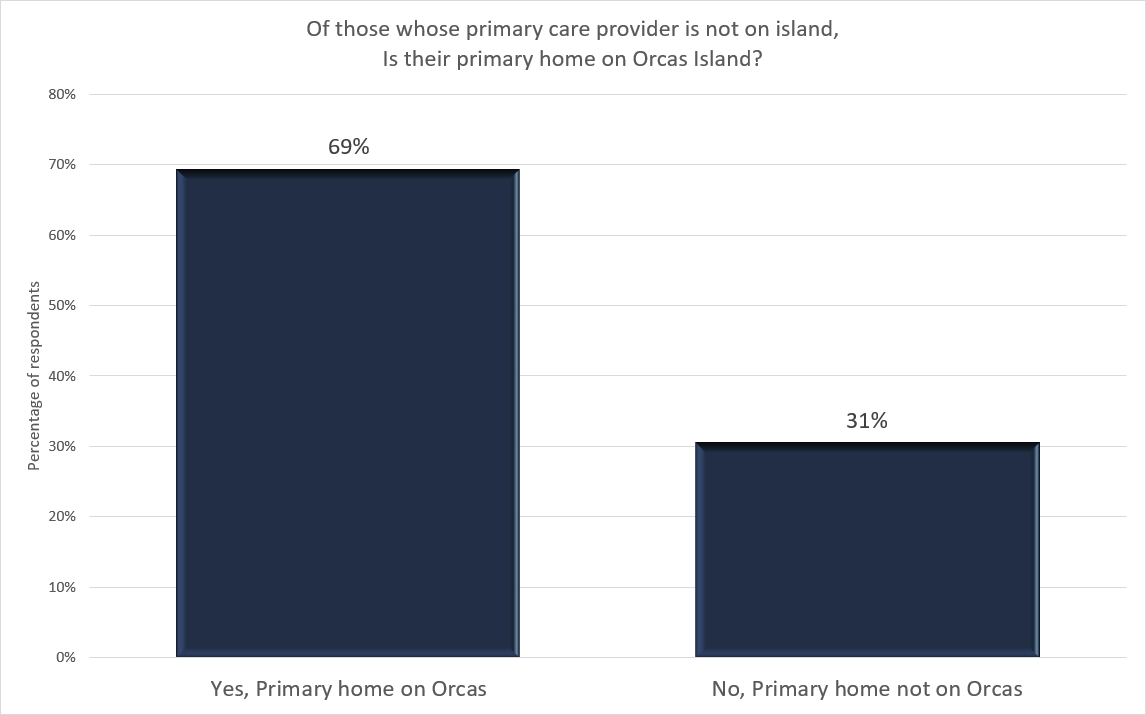
People were asked questions specific to their primary care provider. Those who answered that their primary care provider is off-island were asked two different questions than everyone else: * Is your primary home on Orcas Island? (Yes/No), and, * Why don’t you use one of the island clinics as your primary care provider? (open-ended comment opportunity).
Who we are
Madrona Voices is not associated with the Public Health Care District. Madrona Voices is Steve Smith and Jennifer Smith. We have lived on the island for four years. We live here full time, and we started Madrona Voices because we believe a well-informed and engaged public makes better decisions. We believe that the various boards, commissioners, and councils want to hear from the public but find that difficult to accomplish when many people cannot take the time to participate in the meetings and town halls or read their websites. So, we started doing surveys as another way for the public to be heard. We have demonstrated that we can conduct surveys that are representative of the community, which provides a valuable source of information for all of us. We are at: https://www.madronavoices.com/
Our relationship with those with whom we do surveys
Madrona Voices is independent. We accept suggestions for questions. We accept suggestions for possible answers. We will work very closely with groups that want us to do surveys. As long as we do not detect any attempt to bias the outcome and their desired question style works well with the software we use, we will integrate their requests into the surveys we do. This includes accepting suggestions regarding wording. But, at the end of the day, it is Madrona Voices that accepts and publishes the final wording of the questions and answer options that we distribute.
We have found that the Orcas Island Health Care District commissioners do truly want to know what the community thinks. We detected no attempt to bias the survey in order to elicit any particular response. As a result, we accommodated specific language requested by OIHCD and deleted questions that they did not feel would be productive at this time. This particular survey is very much a joint effort. We know that the OIHCD has been very careful to make sure that the survey was fair to all existing primary care clinics on-island.
How much are we paid?
Madrona Voices does not receive payment or compensation for what we do. We pay for the software and hosting ourselves. We donate our time. We do this as a community service.
Who the OIHCD is
The Orcas Island Health Care District is governed by five commissioners who volunteer a large amount of time to helping the community have the health care it wants. They will use the results of this survey as one of the methods to help them better understand what the community wants and to identify problems that need to be fixed. How they do that involves much more than the survey can cover. You can find OIHCD at: orcashealth.org.
Statement by the OIHCD
The Commissioners of the Orcas Island Health Care District extend our warm thanks to all of you for participating in the recent survey about healthcare services on Orcas. Your thoughtful responses and comments will help guide us as we finalize contracts with the clinics for the next year and help us set priorities for the future.
Shortly after the District was formed, the Board began discussing how to engage with the Orcas community to make sure that we hear from a larger portion of the community than the few who seek us out individually or attend our meetings. We decided that the best way for us to hear from more of you was through a combination of town hall meetings and short, focused surveys.
The primary focus of the survey was to learn what kind of acute care services the community wants and test the
community’s willingness to pay more in taxes to receive those services. Additionally, we wanted to gauge satisfaction with the medical care currently available on Orcas to help guide our discussions in negotiations with the clinics.
The Board asked Madrona Voices to conduct the survey because of their experience conducting several surveys on local issues on their own initiative. By collaborating with them, the Board was able to have some influence over which questions were asked and how questions were phrased. However, because the survey was conducted by Madrona Voices, they retained control over how and when the results were presented and what was made publicly available, including the comments.
We thank you for your candid feedback which we will use to prioritize our interactions with the clinics to improve the services they offer. We also provided each clinic with a copy of the compiled survey responses and the text of the comments.
Again, thank you very much for taking the time to complete the survey. We appreciate your input.
Statement by Madrona Voices
As some may know, on this particular survey, there was some discussion at OIHCD meetings about whether or not we should publish the comments, as is our practice at Madrona Voices. We decided to publish them primarily because we told the community that we would. We sent all respondents an email after they took the survey, reminding each that we would publish all results, including the comments. We were encouraged to send this reminder by those we collaborated with. We believe that the comments, over all, are helpful in identifying what is and is not working well in regards to healthcare on the island. As humans, our own health and the health of those we love matter a great deal, so the topic naturally prompts several passionate statements about experiences. One can learn from all comments, both about what is happening for most as well as what is happening for each individual. One can see where better communication or service is needed. Some comments are emotion-packed. That is to be expected and understandable. It is an emotional topic that goes deep for everyone on a personal level. As a community, we tend to want to take care of each other, and that is often why people are drawn to rural settings or even small, intimate gatherings in urban settings. People need each other, no matter where we are. You’ll see the roots of these concepts in the comments.
In working with the commissioners on this survey, we believe that they do welcome the feedback and are doing their very best to work in the best interests of the community. They have compassion for those needing the health care as well as for those who are serving others in the healthcare field. We are thankful for all they do for the community. We encourage you to see their website for contact information and their own perspectives: https://orcashealth.org/
As always, we appreciate your participation in our surveys.
Executive Summary
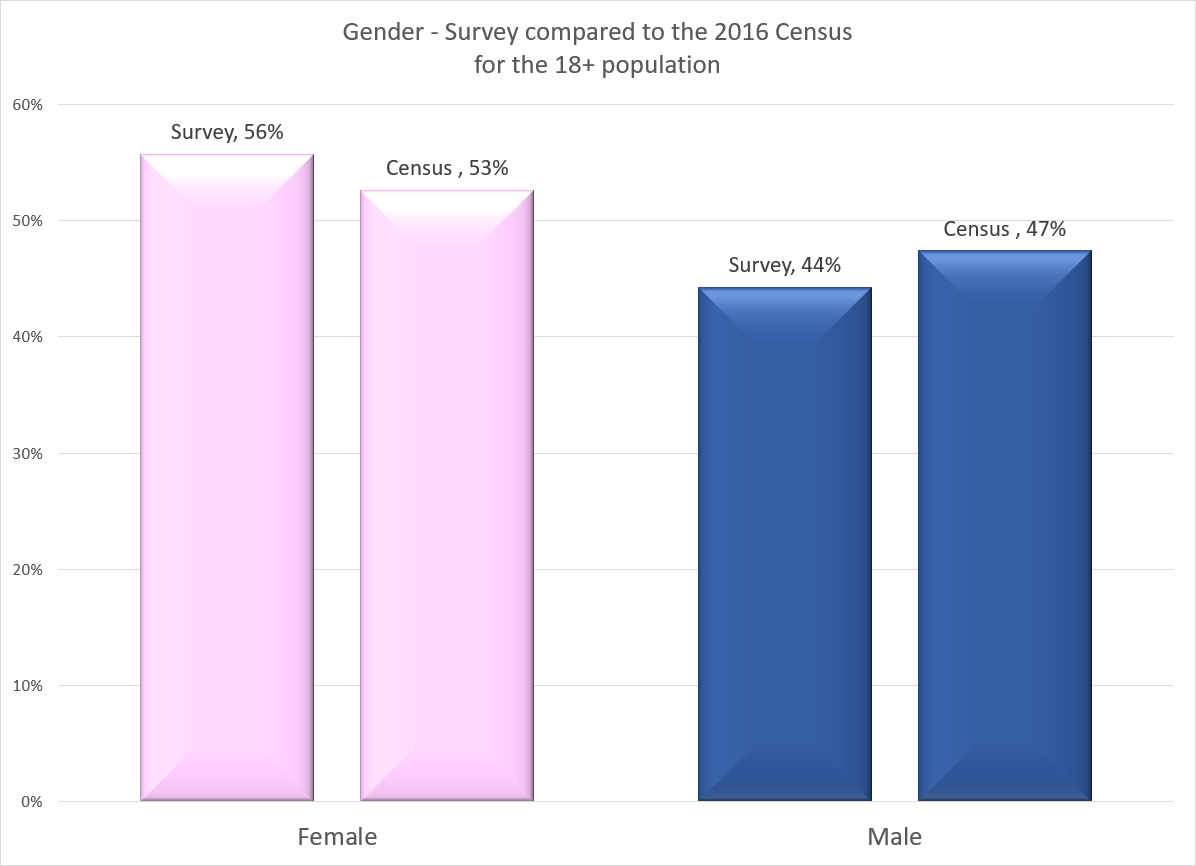
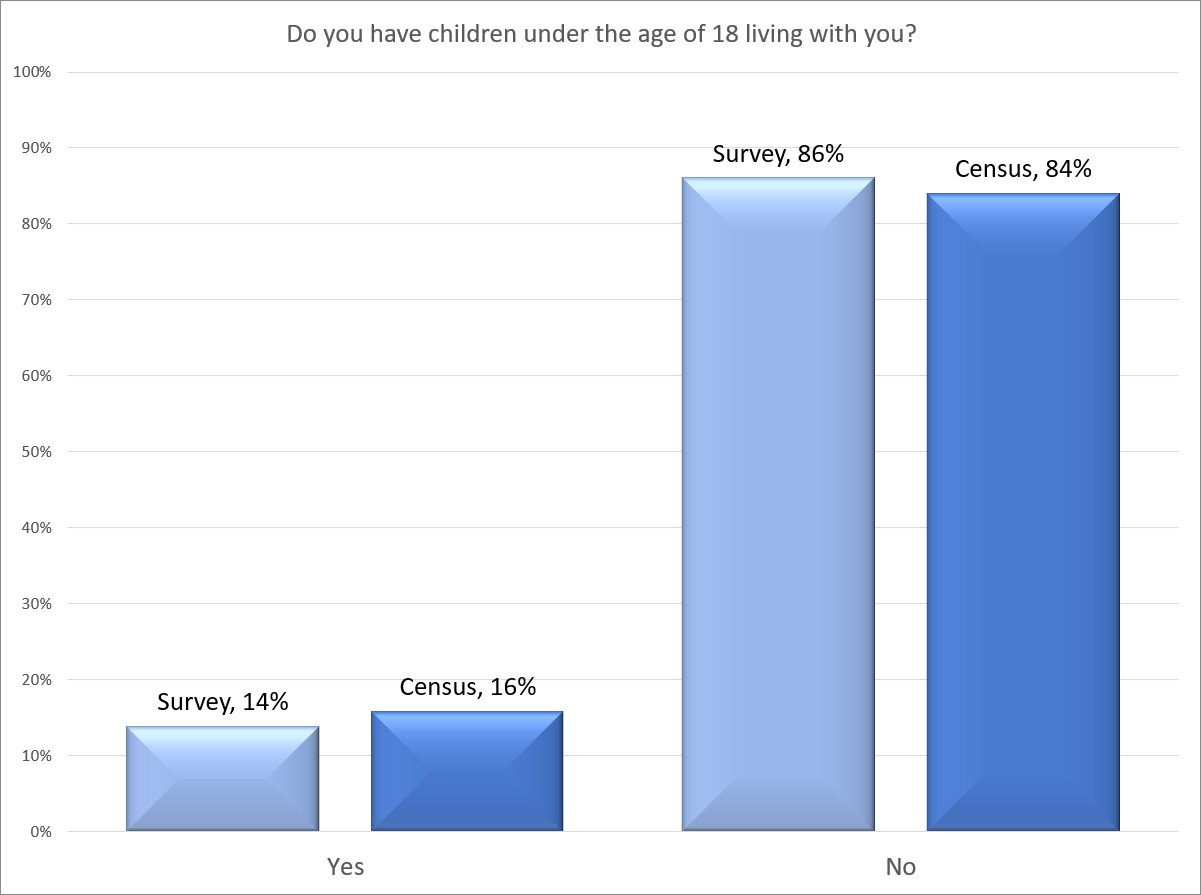
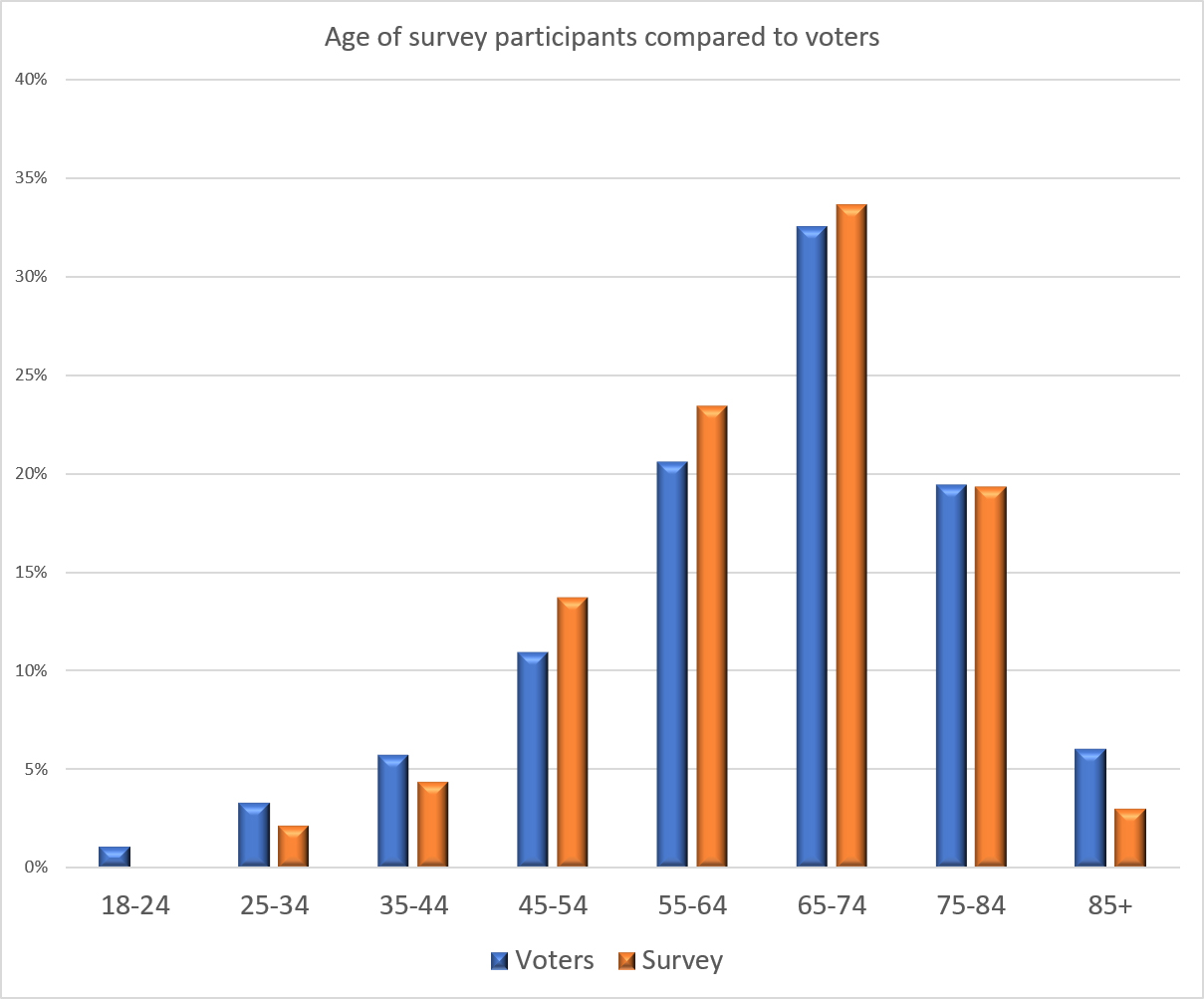
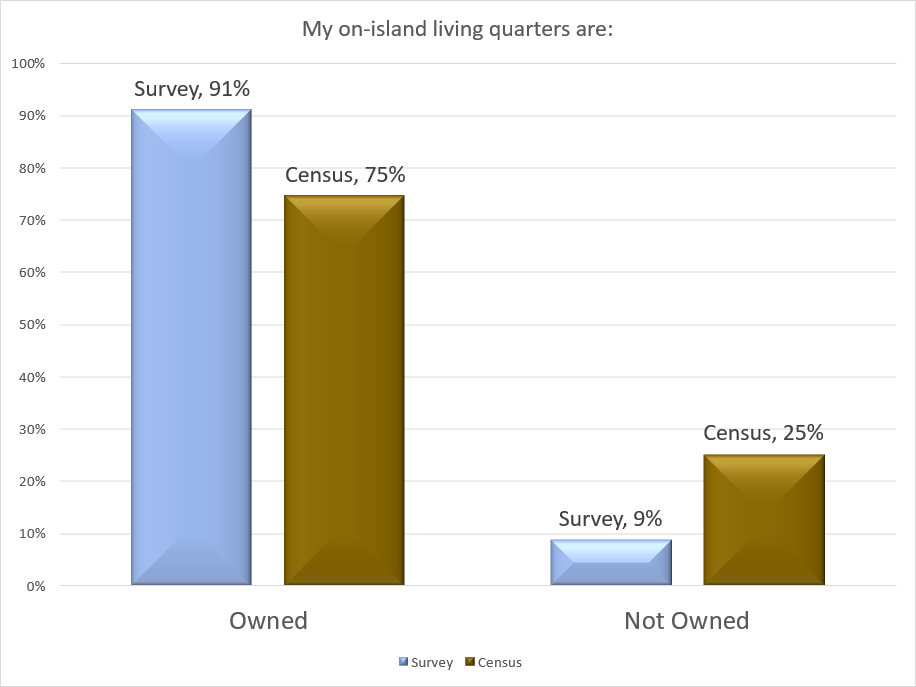
Over a two and a half week period, we at Madrona Voices received responses from 640 participants with 1,370 comments. The participants represent more than 13% of the adult population of the island. We closely match the demographic profile of the community by gender, households with children, and the age profile of voters. We under-represent renters; however, the renters who participated in the survey share the same opinions on policy questions that participating homeowners do in the survey. As a result, we do not under-represent the opinions of renters. Please see Appendix A for a more detailed review.
Some overall facts based on what respondents shared in this survey:
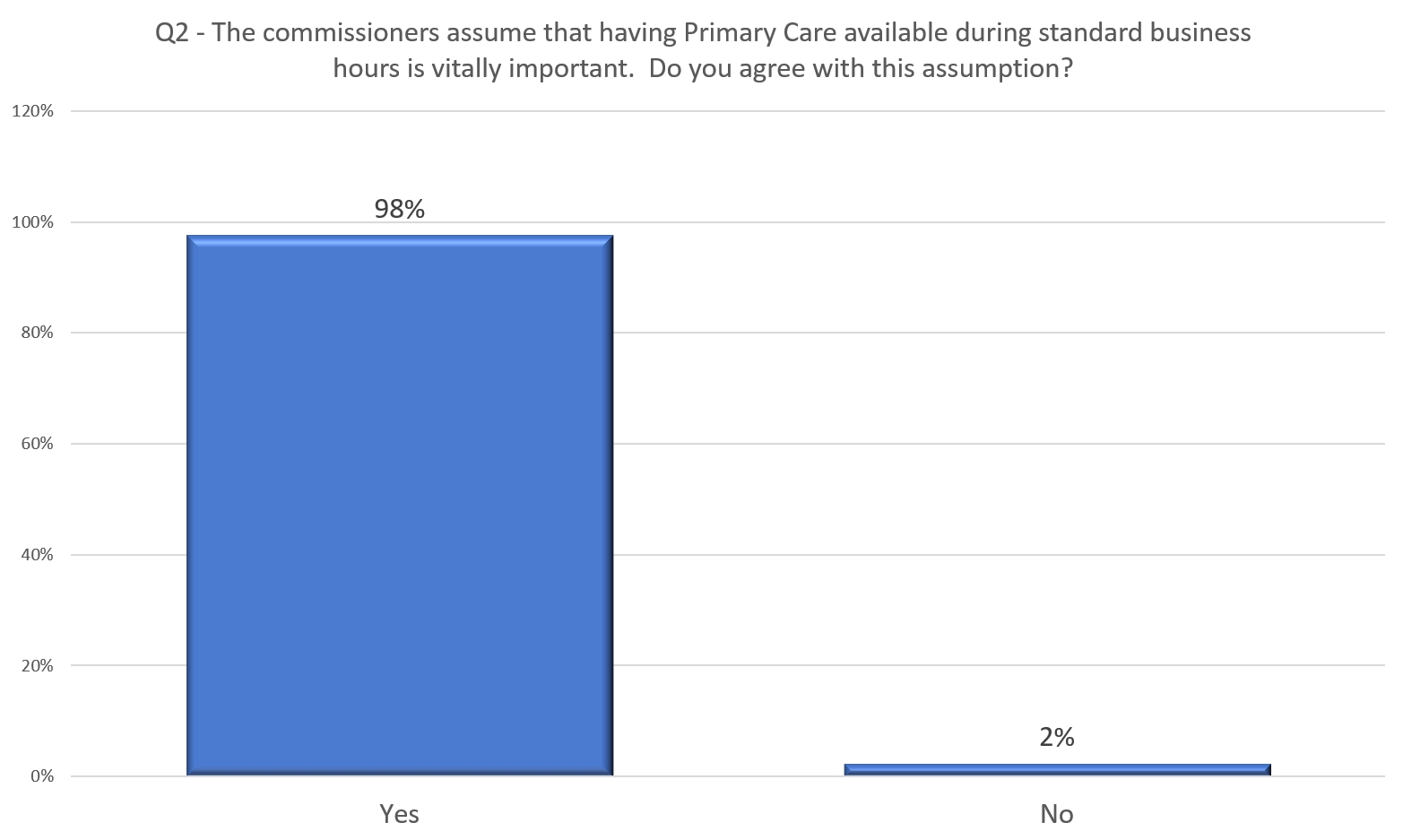
- The community almost universally agrees with the commissioners’ assumption that primary care is vitally important to the island.
- The majority likes the idea of increasing clinic access.
- A slim majority wants non-urgent appointments to be available within one week of calling.
- The vast majority wants non-urgent appointments to be available within two weeks of calling.
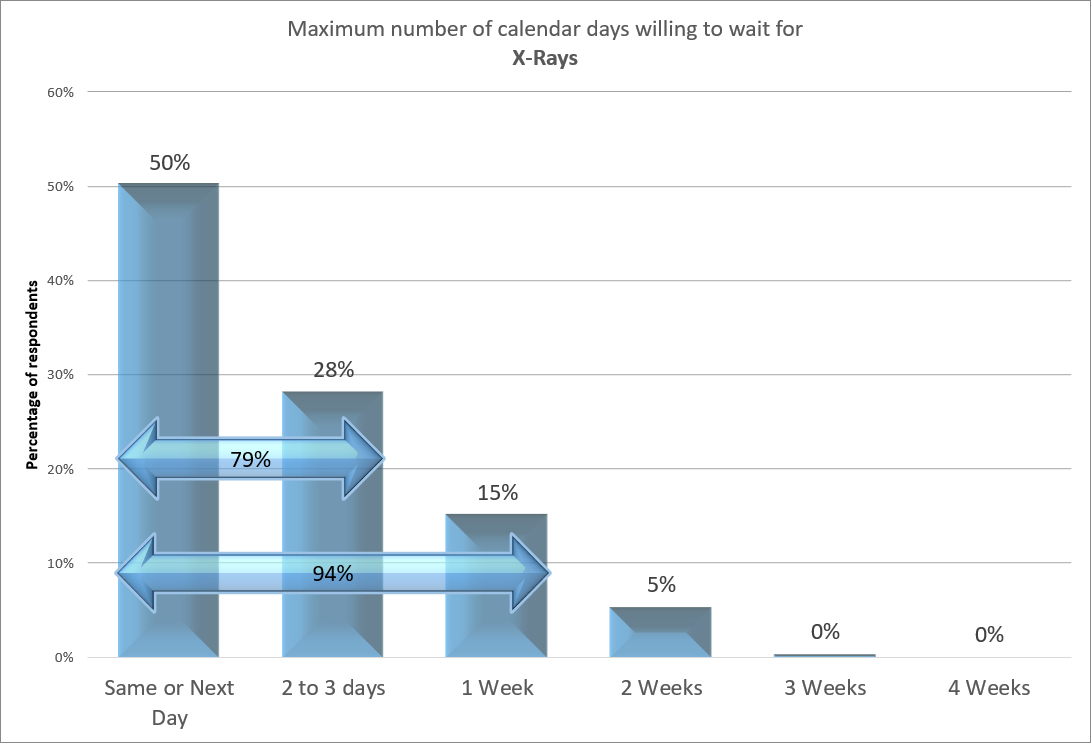
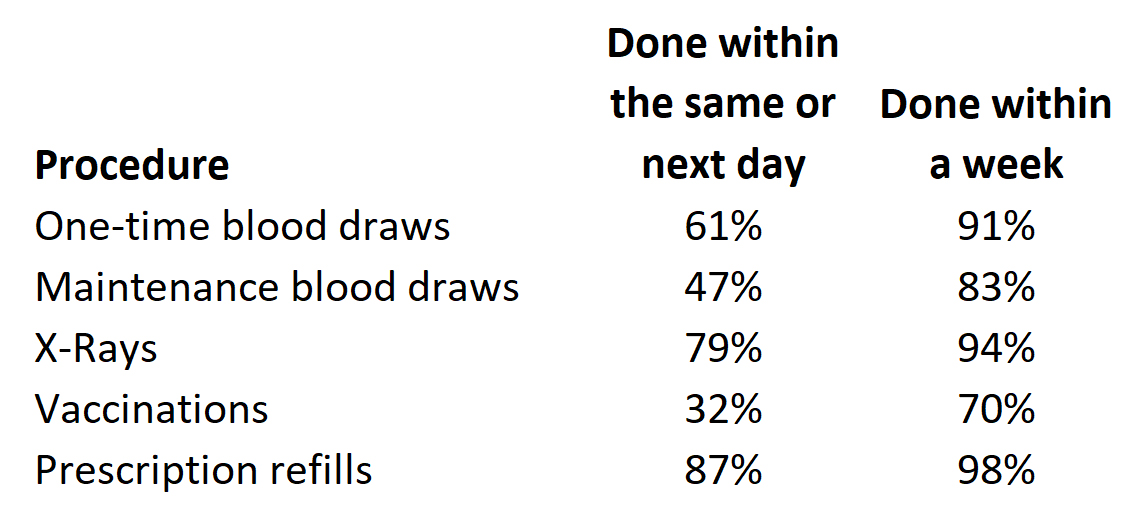
- A majority wants X-Rays and prescription refills to be available the same or next day.
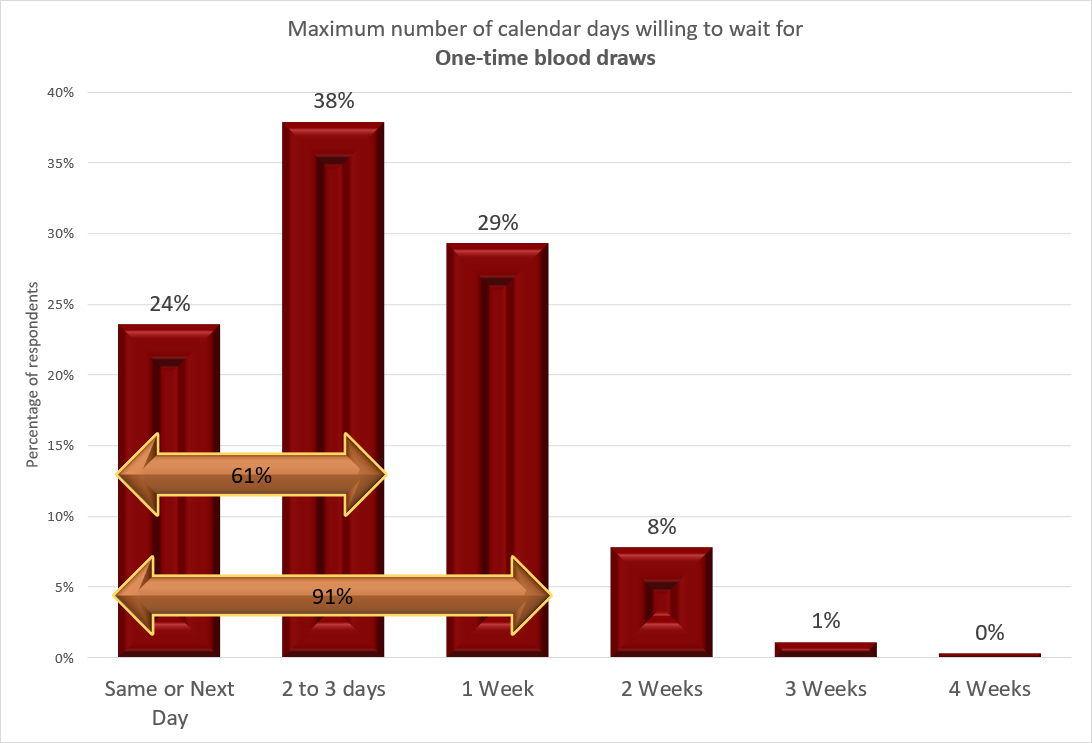
- A majority wants one-time blood draws within 2 to 3 days.
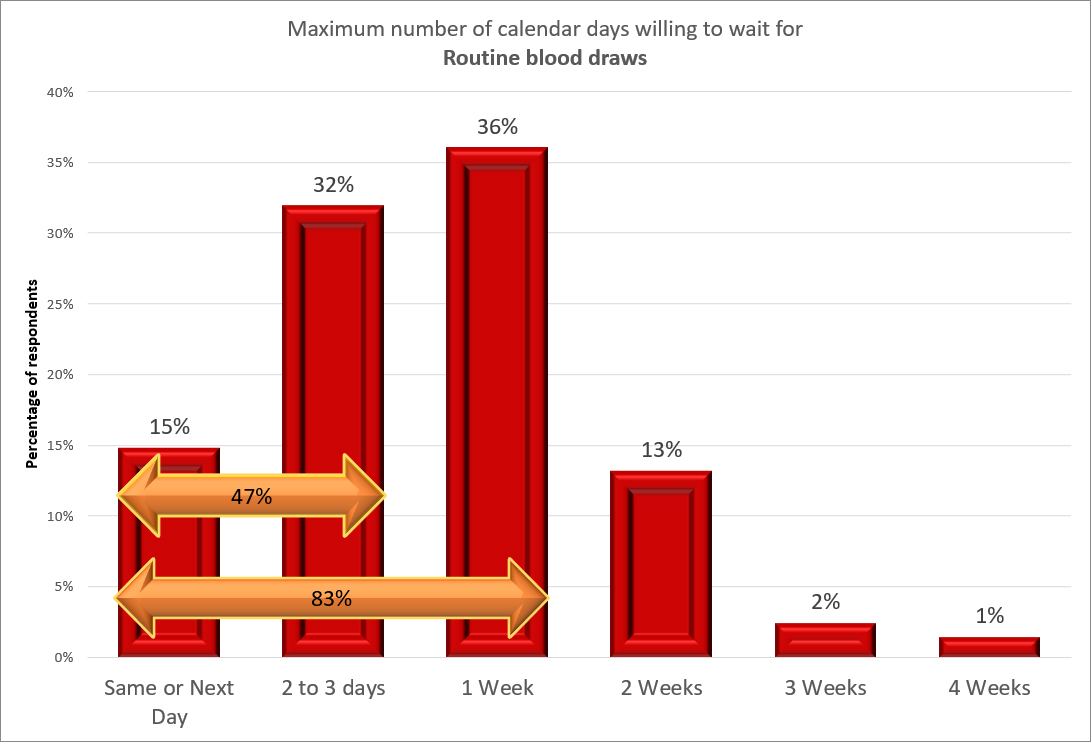
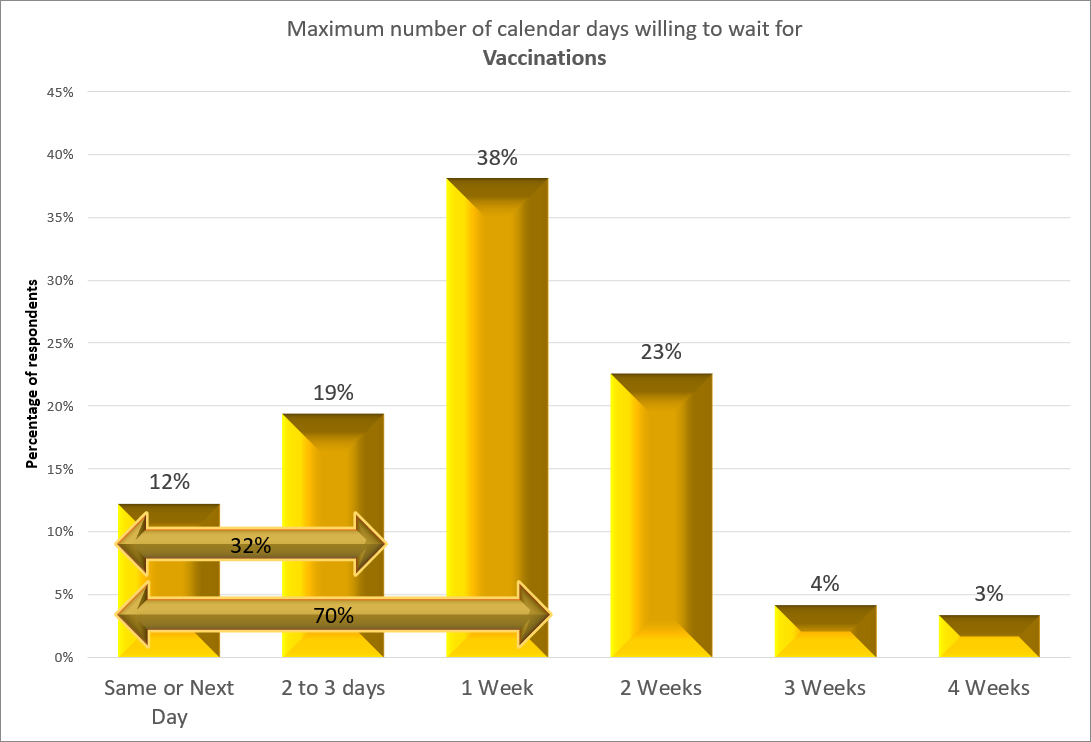
- A majority wants maintenance blood draws and vaccinations to be scheduled within a week.
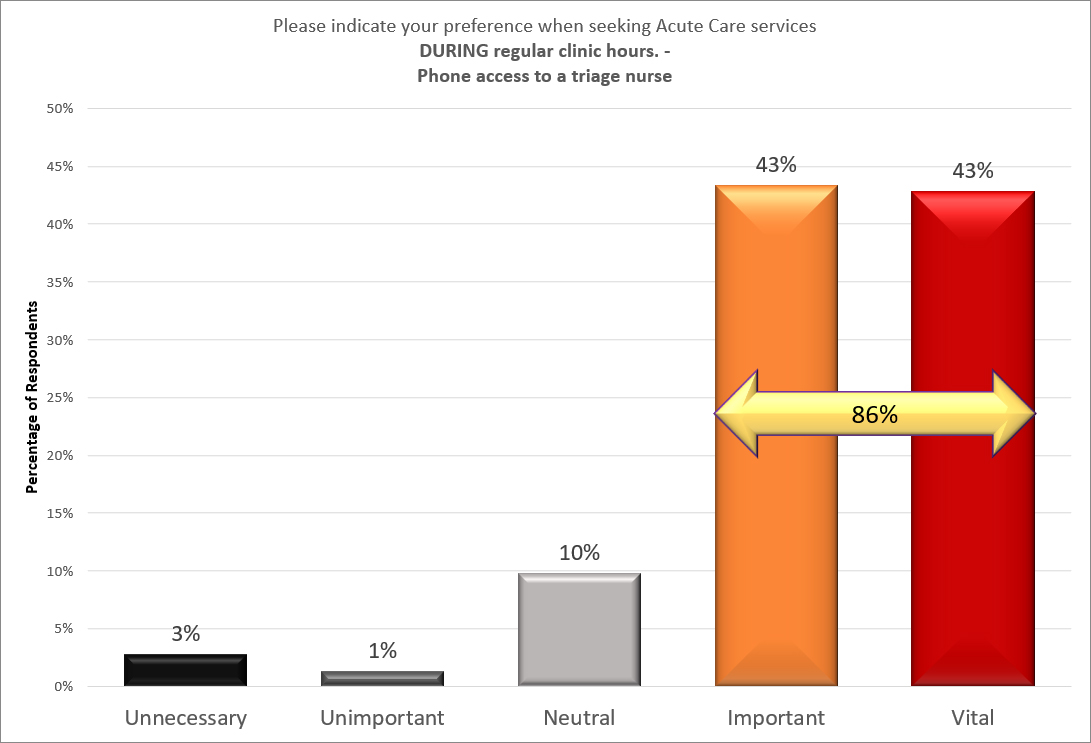
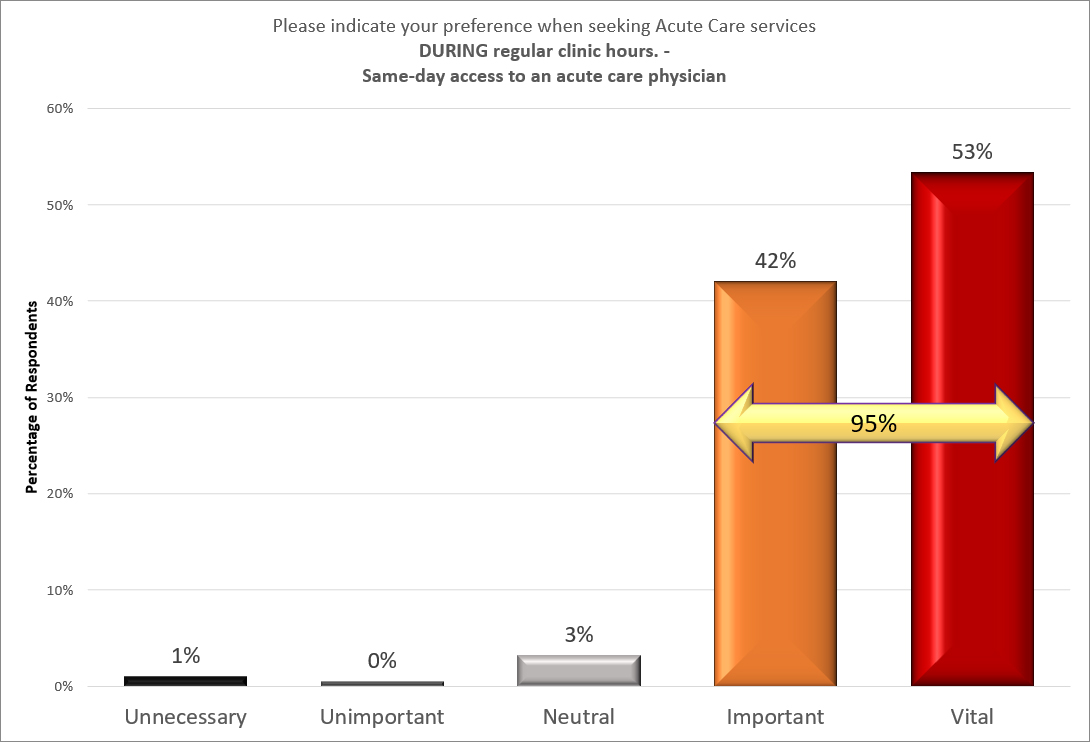
- There is overwhelming support for Acute Care services in the form of a triage nurse and access to a medical provider being available during clinic hours.
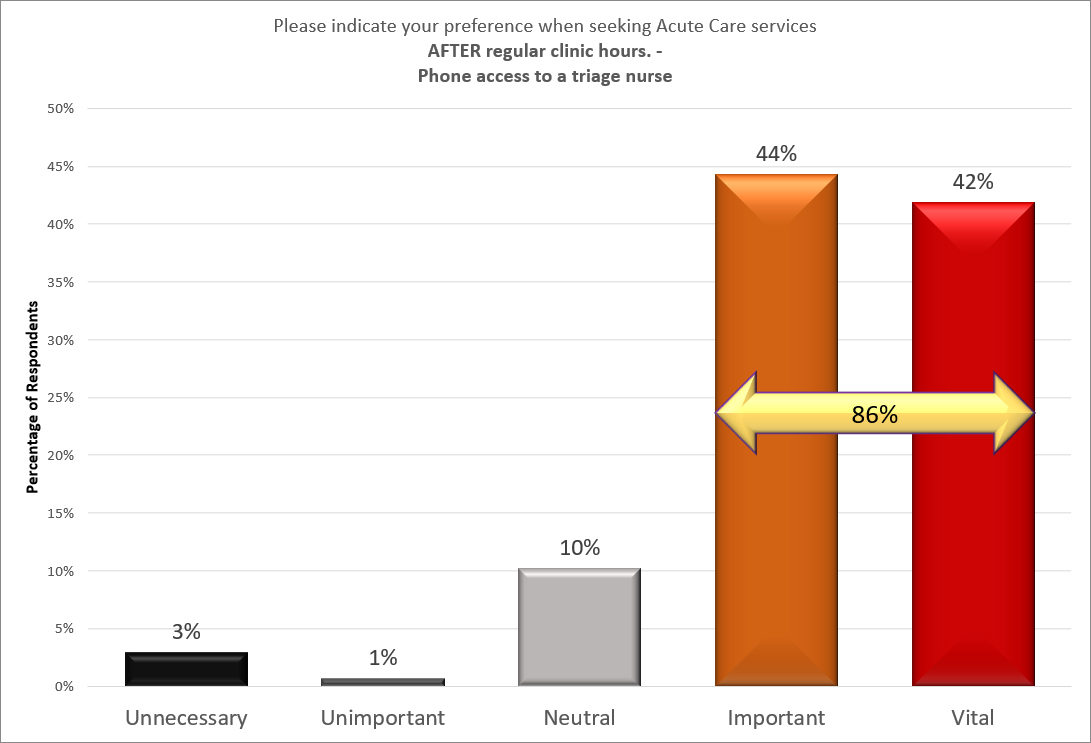
- There is also overwhelming support for the same Acute Care services after-hours.
- A very large percentage wants Acute Care services to be available to everyone, whether they are a resident or visitor.
- Respondent patronage by provider is:
- 52% UW
- 29% OFHC
- 12% Off-island
- 6% No primary care provider
- 2% Other island provider
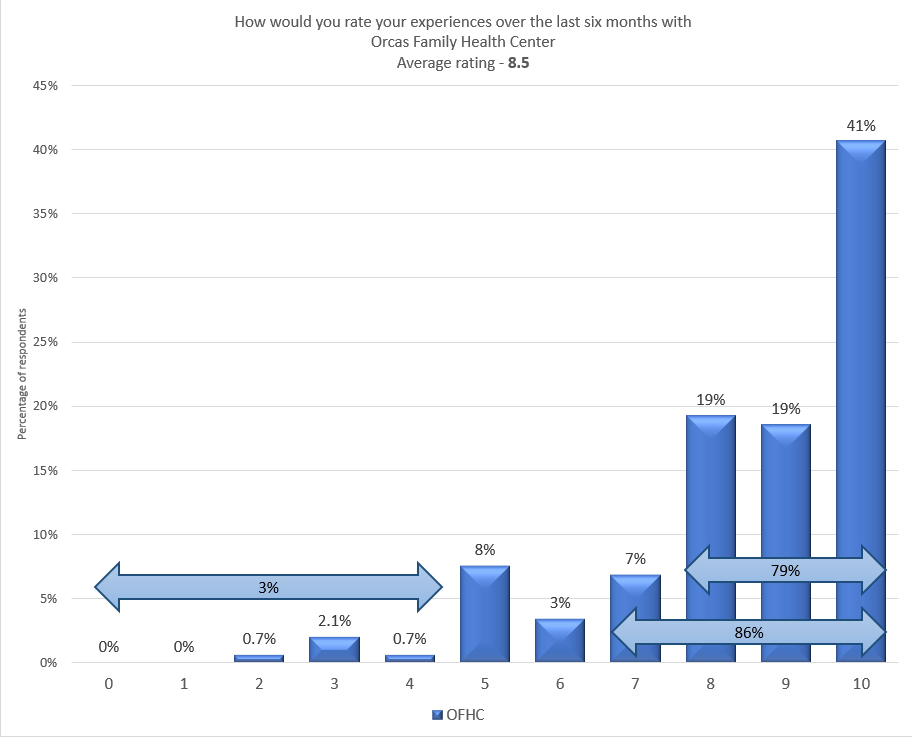
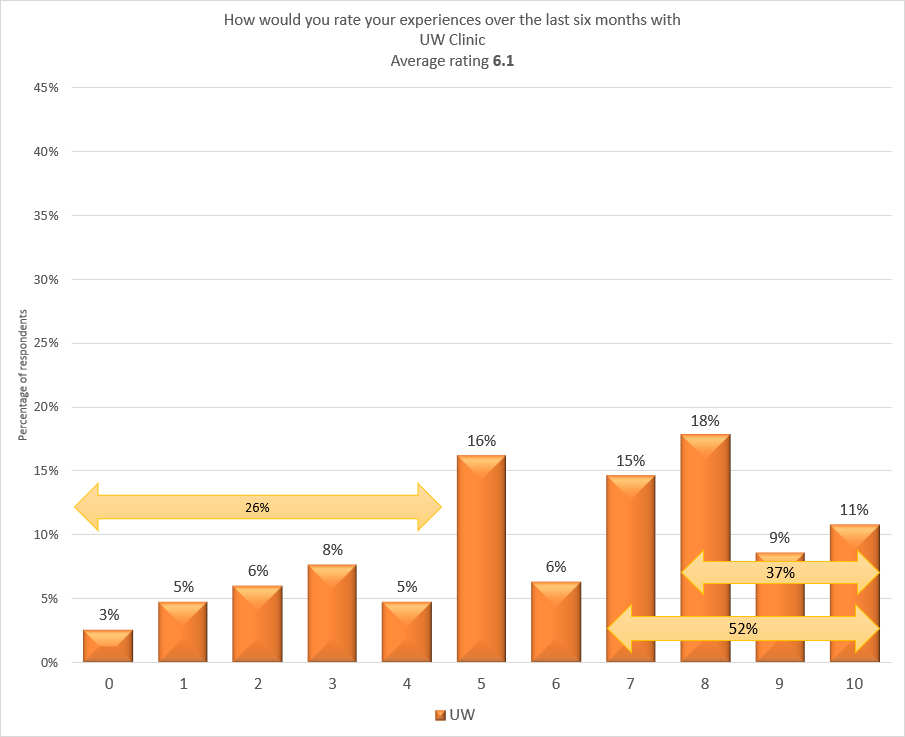
- There is a difference in the satisfaction level with OFHC and UW. Patrons of OFHC are more satisfied with service in the last six months than are the UW patrons for service there in the last six months.
- 79% of OFHC patients give their clinic a rating of 8 or higher.
- 37% of UW patients give their clinic a rating of 8 or higher.
- This survey is representative of the community. See Appendix A for details about how we determine this.
In summary, the primary findings are that the community wants medical service in a timely fashion. The community wants Acute Care, both during clinic hours and after-hours. The satisfaction level with the clinics is higher with OFHC than with UW. Health care on Orcas is an important issue about which many are concerned and want to communicate. We thank the Orcas Island Health Care District for choosing Madrona Voices in providing another opportunity for the public to communicate those concerns.
Question Format
The form of the question varied by the device that the participant was using.
We test each question to make sure that it is readable on desktops, tablets, and phones.
Viewing hints while reading this report
You can click on all images to make them larger. You can click on the back arrow to exit the enlarged graph. Some of you may experience problems using the back arrow. An alternative way to see the image larger is to right click on the image and open it in a new window. Then, close that window when finished viewing.
For Mac users: Cmd ⌘ Click will open a link in a new tab behind the current one, if you click a link. Cmd ⌘ Shift ⇧ Click will open the new tab & bring it to the front. Close that window to return to the report.
It is a trade off between making the images readable on small screens and letting you see them full size, if you need to.
Question Responses
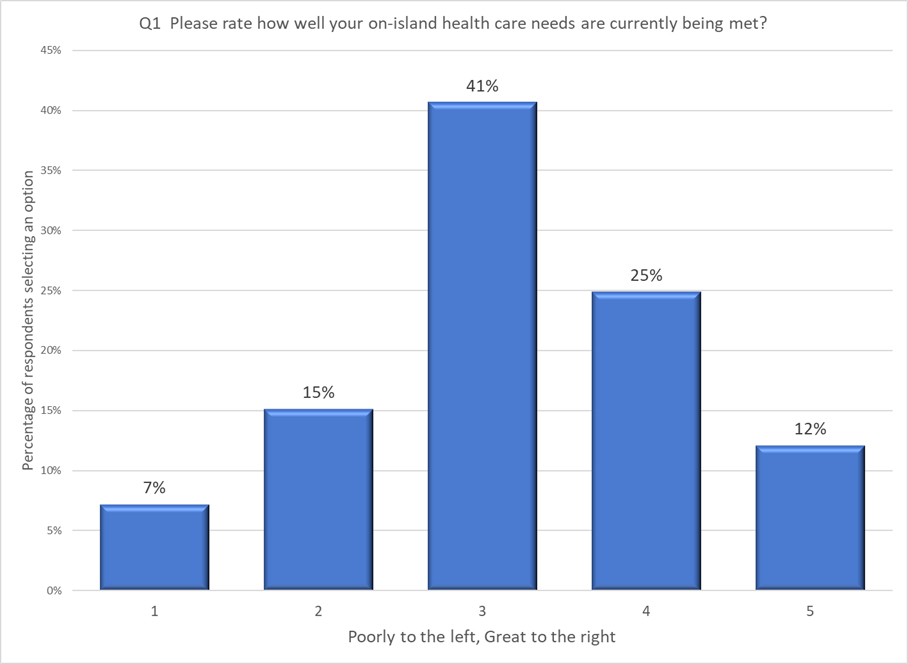
Q1 – Please rate how well your on-island health care needs are currently being met?
The first question is our “hook.” It is the question we embed into the email invitation that we send to everyone. A person was allowed to select one to five hearts, with one heart being labeled “Poorly” and five hearts being labeled “Great.” There are five steps.
Q2 – The commissioners assume that having Primary Care available during standard business hours is vitally important. Do you agree with this assumption?
Q3 – Easier access to clinics
Each row is a different issue.
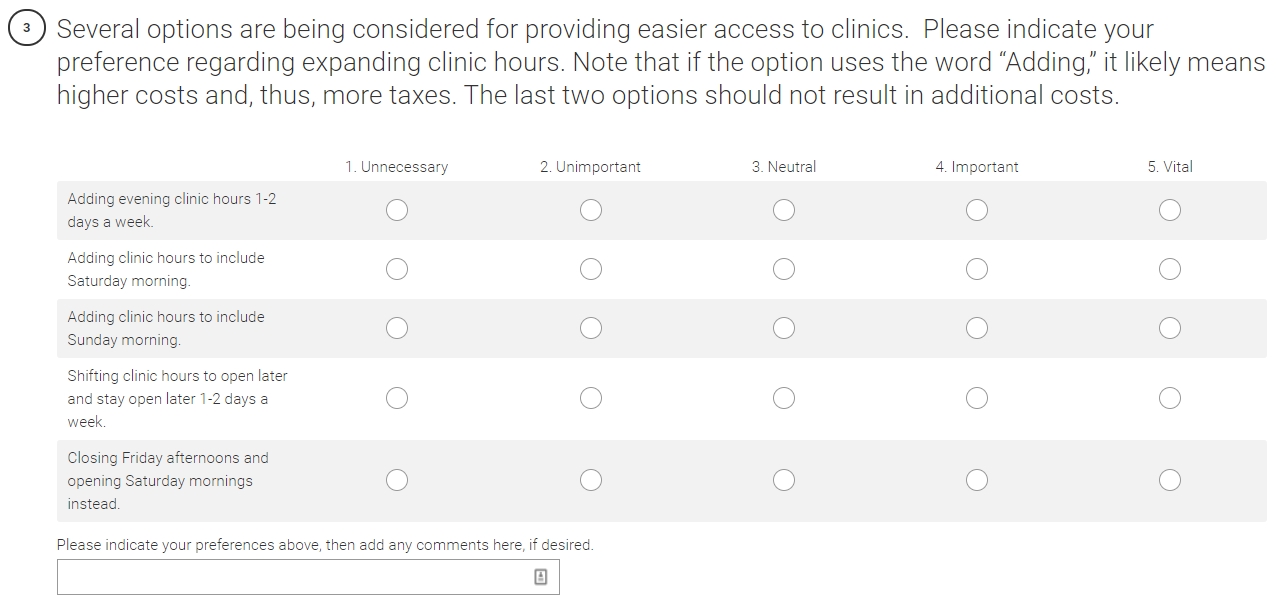
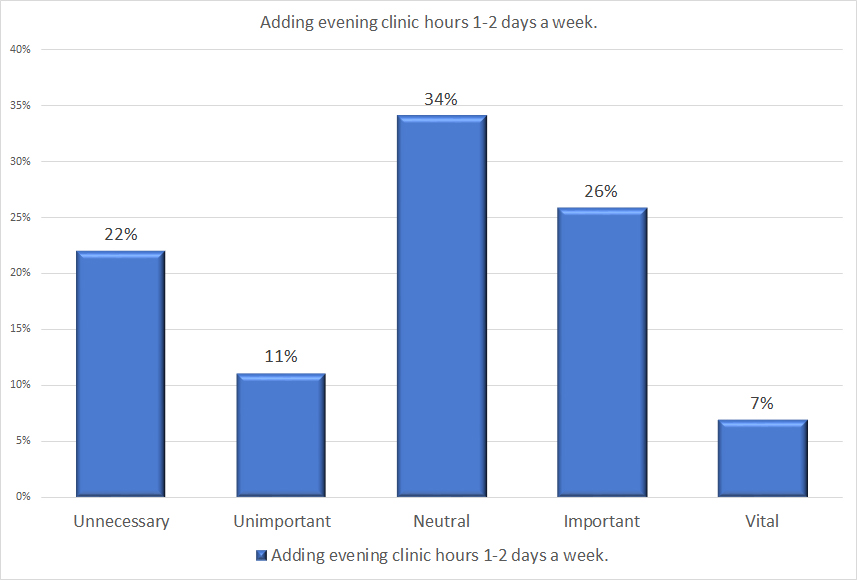
Q3a – Evening access
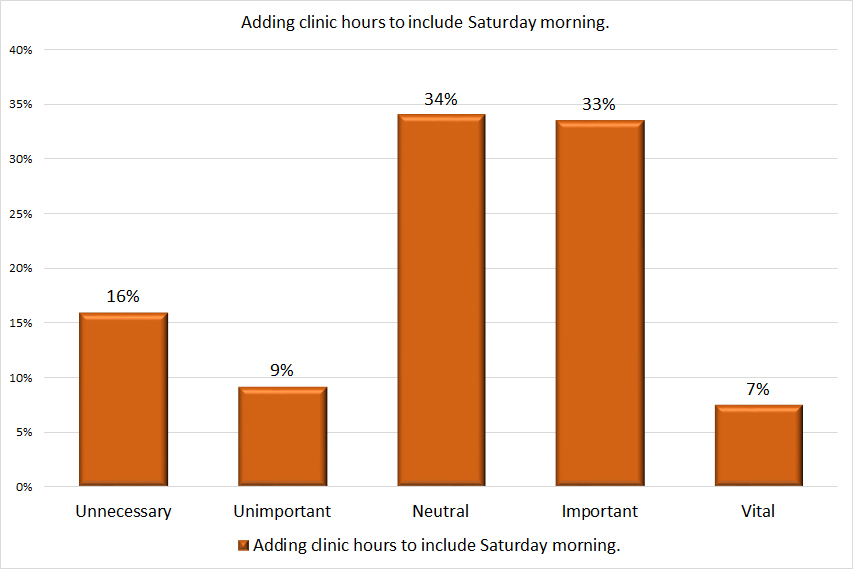
Q3b – Saturday morning hours
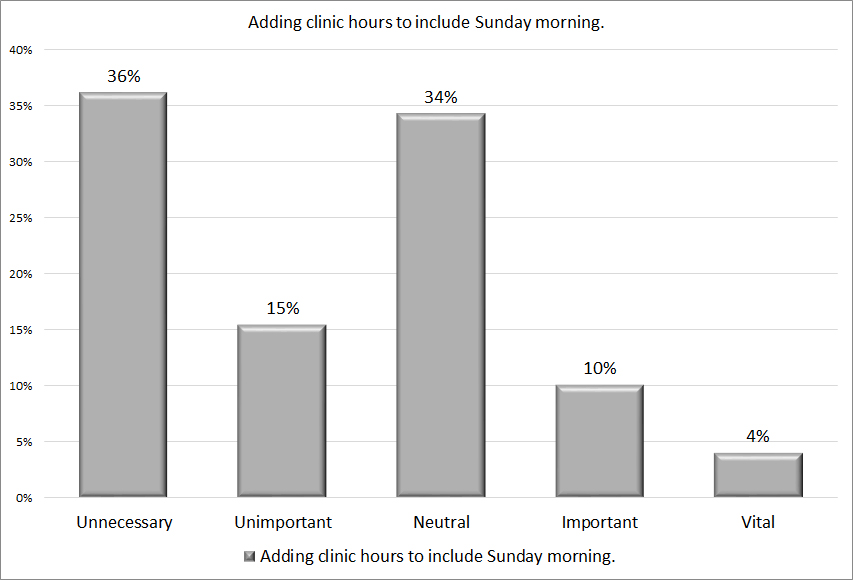
Q3c – Sunday morning hours
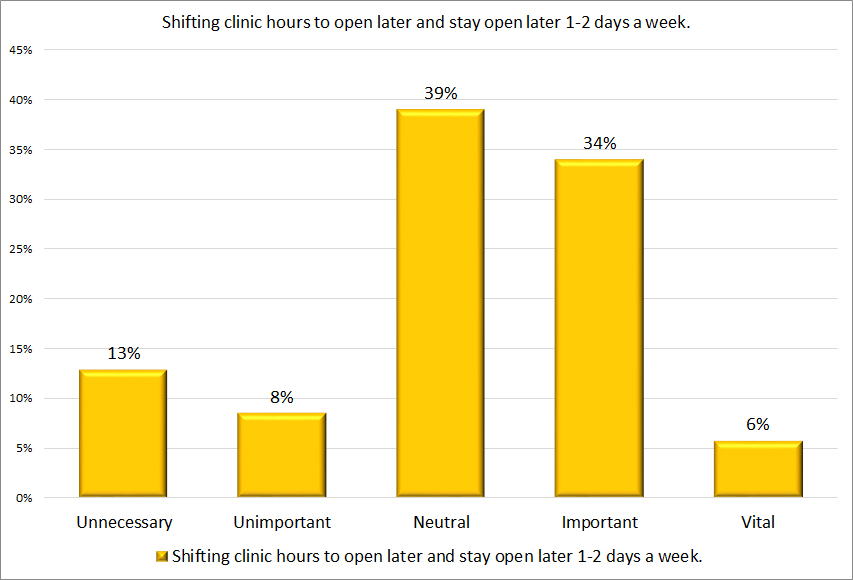
Q3d – Shifting hours
Q3e – Shifting days
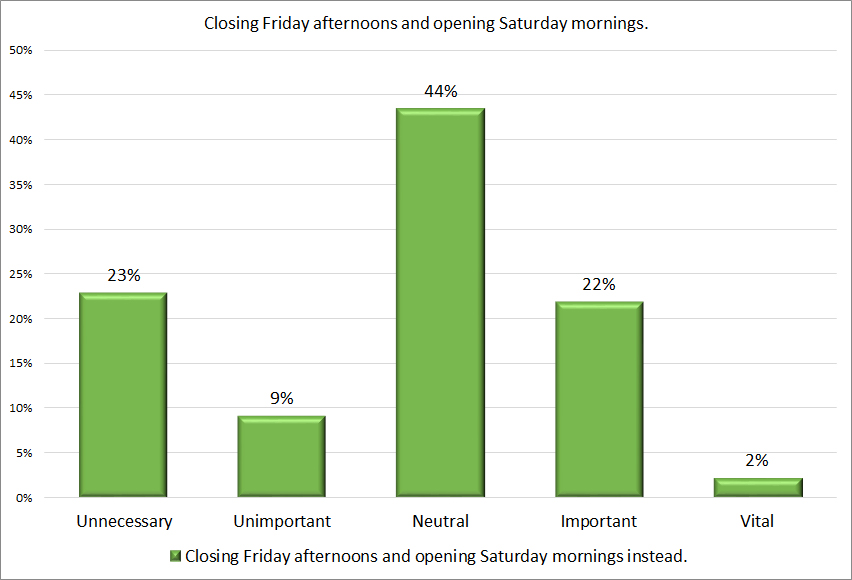
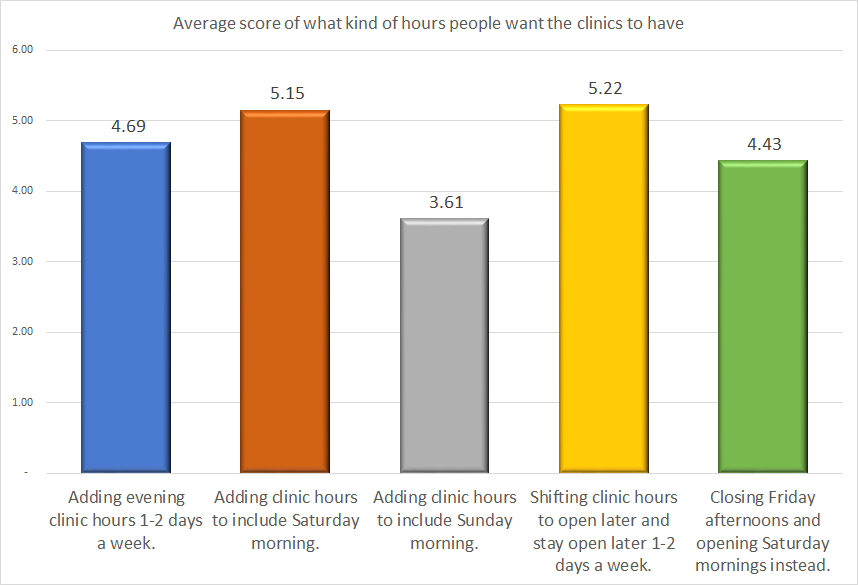
Q3 Options Compared
Q3 – Least necessary
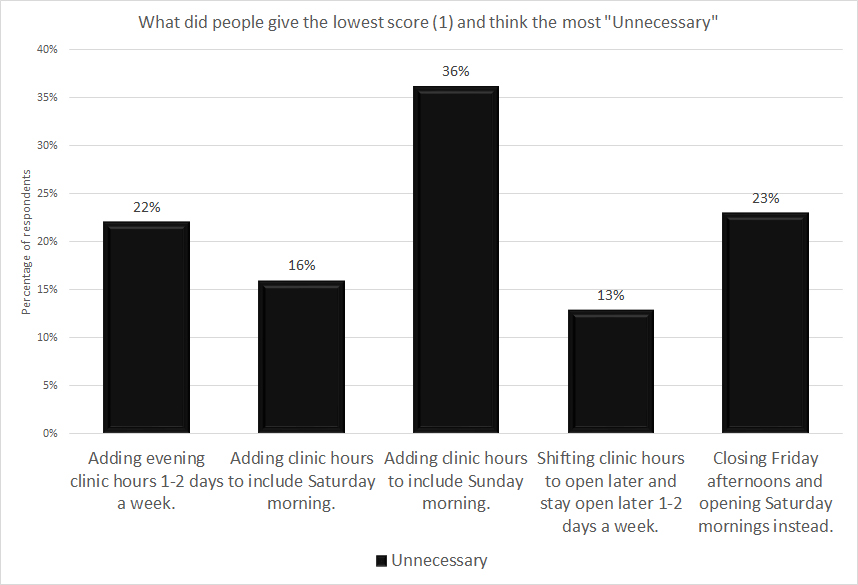
The higher the black column, the less people think they need it. The lower the bar, the more people think it is helpful.
The least popular option of the five is adding clinic hours on Sunday. Shifting clinic hours is the most popular, closely followed by adding clinic hours on Saturday morning.
Matrix Scoring Formula
The formula for determining the numbers associated with each option is:
w = weight of answer choice
x = response count for answer choice

The weights we used are:
- 1 – Unnecessary
- 3 – Unimportant
- 5 – Neutral
- 7 – Important
- 9 – Vital
The greater the difference in the weights, the more exaggerated the differences between columns. However, the proportion of the differences remains the same.
Q3 – Increasing Access Comments
We provided opportunity for people to comment on the various ideas for increasing access. Click here to read the respondent’s comments about Increasing Access.
Q4 Maximum number of calendar days until an appointment
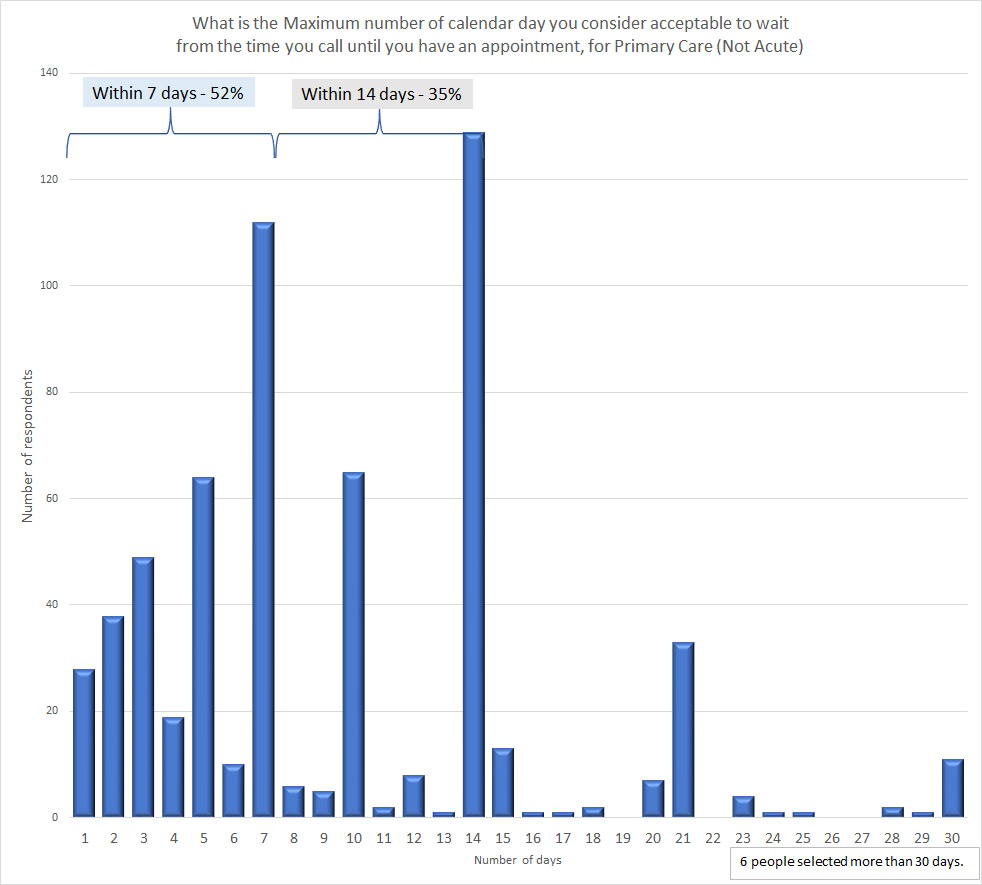
We allowed people to select between 1 and 45 calendar days for the maximum amount of time that a person is willing to accept from the time that they call for an appointment until they are able to have the appointment. Over half of respondents (52%) considers the maximum acceptable wait time to be seven or fewer calendar days. The large majority (86%) considers the maximum acceptable wait time to be 14 calendar days or less.
Six people selected more than 30 days, which we do not show on this graph.
Q5 – Maximum acceptable time for various procedures
The question as it appeared in the survey.
Q5a – One-time blood draws
Q5b – Maintenance blood draws
Q5c – X-Rays
Q5d – Vaccinations
Q5e – Prescription Refills
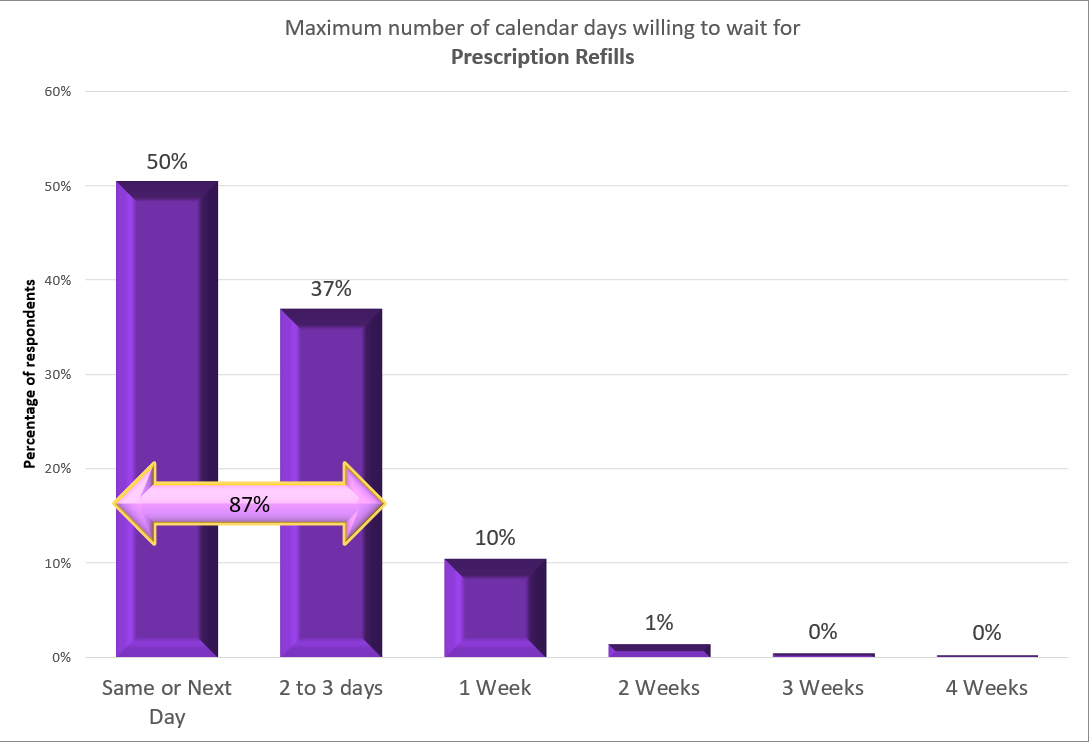
Q5 Summary
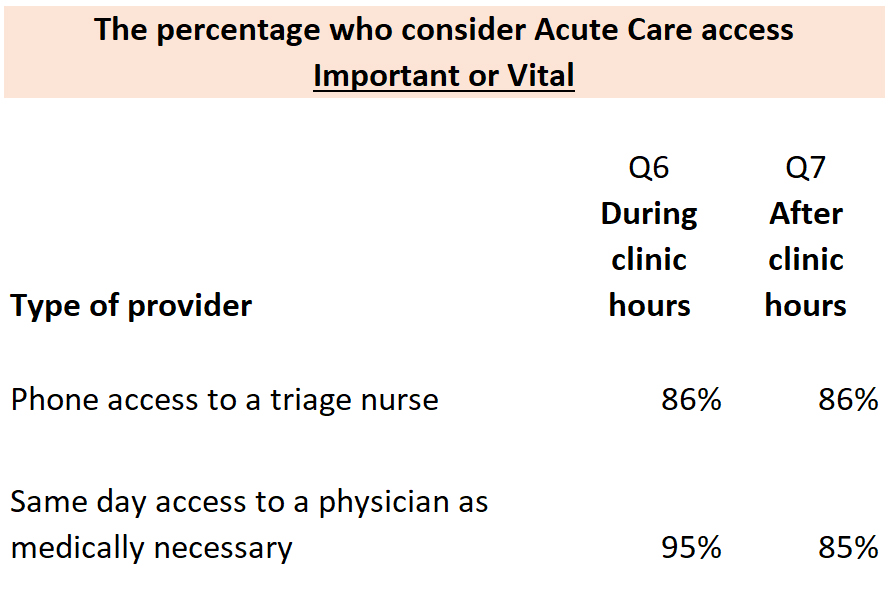
Q6 – Desire for Acute Care DURING clinic hours
Format for Questions 6 and 7 about Acute Care both During and After-Hours.
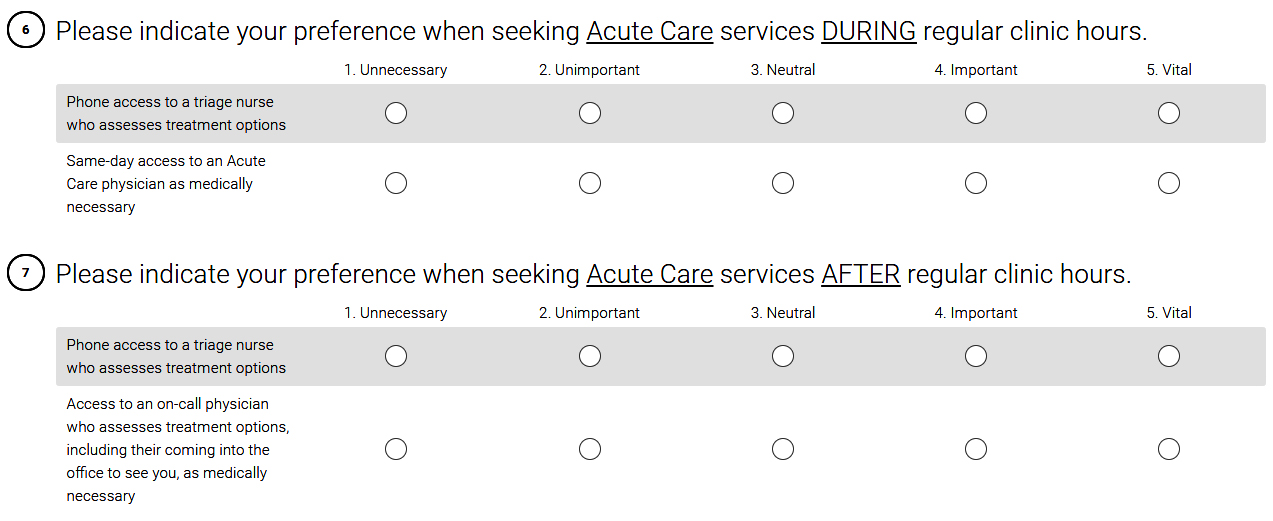
Q6a – Triage Nurse DURING clinic hours
Q6b – Acute Care Physician DURING clinic hours
Q6c – Triage Nurse AFTER clinic hours
Q6d -Acute Care Physician AFTER clinic hours
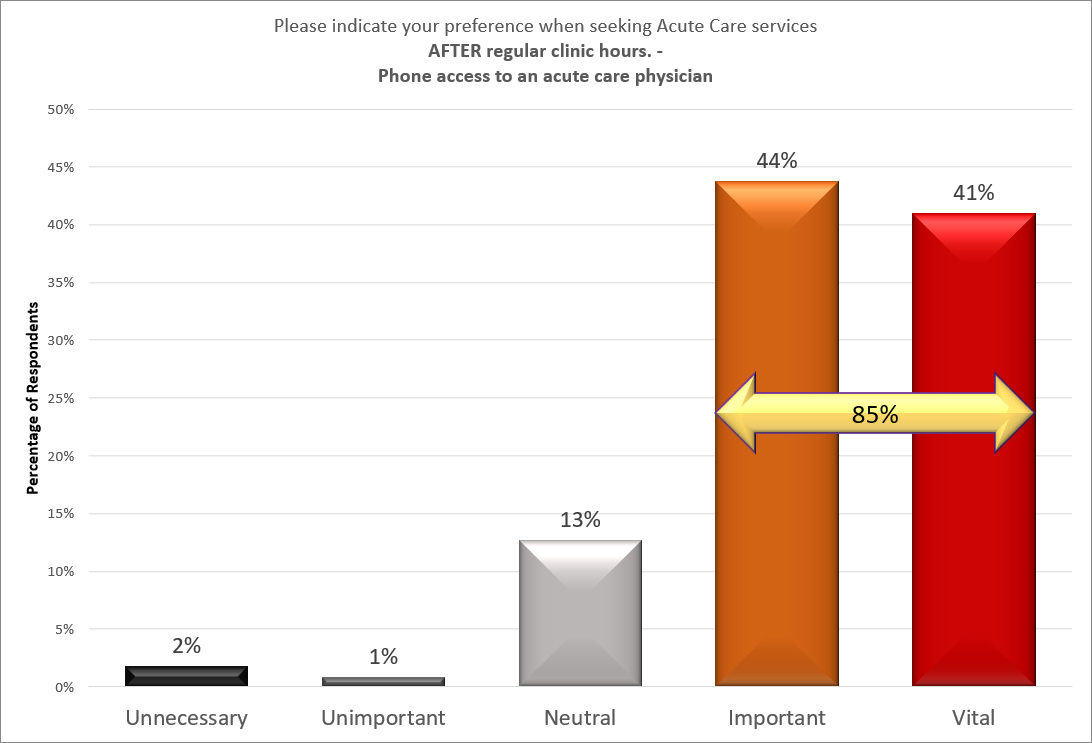
Q6 and Q7 Summary
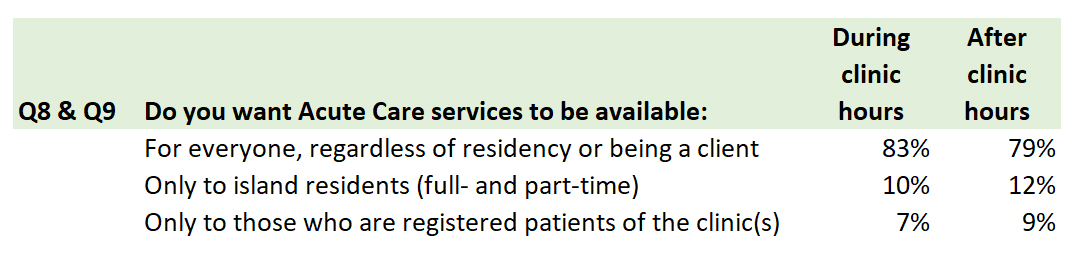
Q8 and Q9 Summary
Comments about who receives Acute Care During clinic Hours
Comments about who receives Acute Care After clinic Hours
Q10 & Q11 Question Format
A person could slide the dot or type a number into the box to select an amount between $0 and $15.
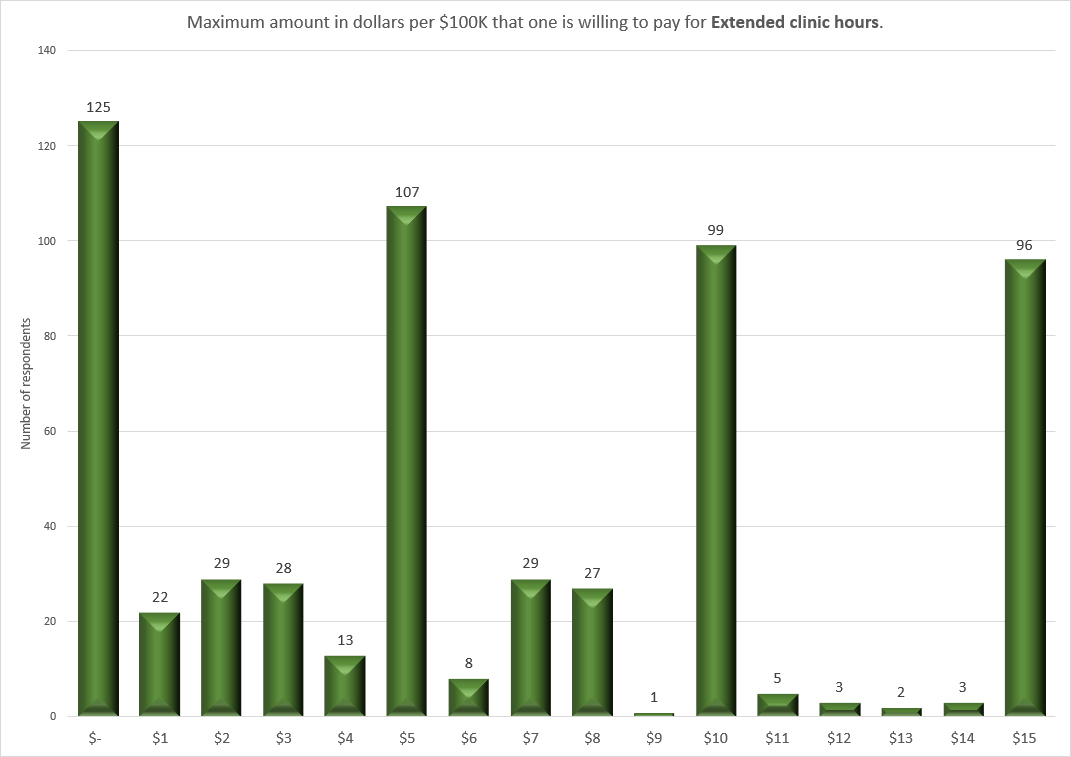
The following two graphs show how many people selected each option.
Q10 – Taxes for extended clinic hours
We considered a number of ways of shading or grouping different time periods. But, every grouping has its own bias. So, we decided to just present the raw information and let you decide which columns to add together, if any.
Q11 – Taxes for extended After-Hours care
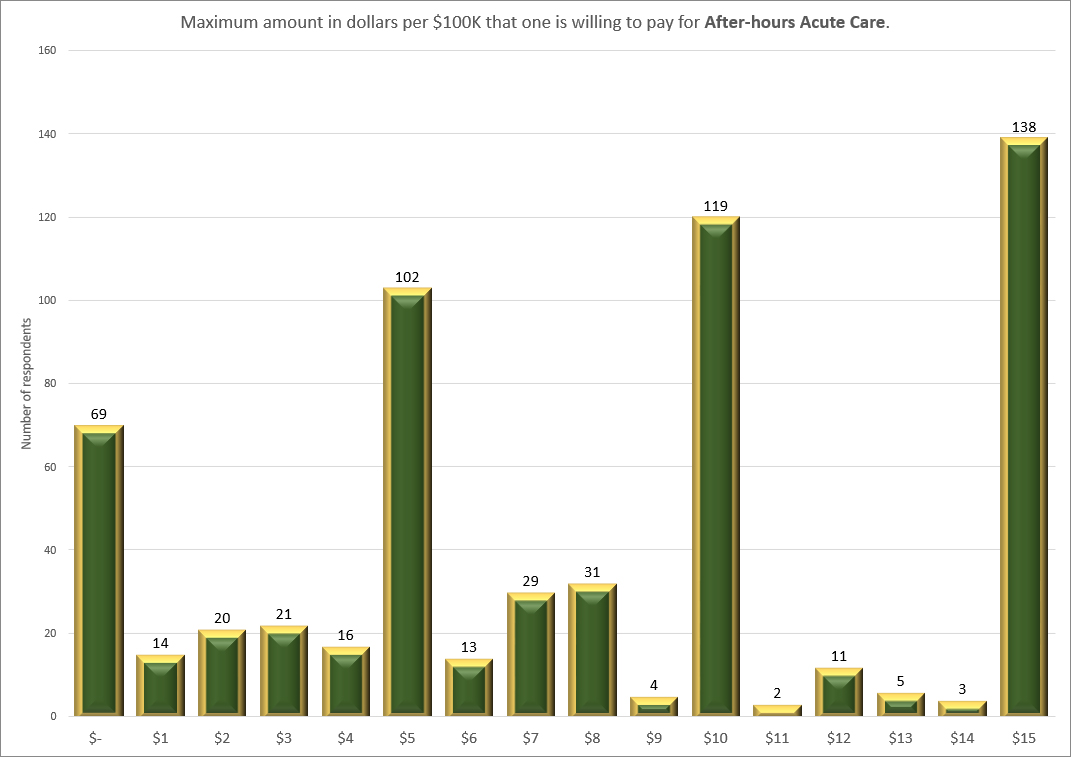
Note that if the commissioners have $15 per $100,000 in property valuation that they are considering using for extended hours or for after-hours care, then the combination of the two questions cannot add up to more than $15. If the commissioners allocate $15 for one idea, they won’t have any money left to allocate for the other idea.
People are more willing to see more tax dollars spent on after-hours Acute Care than they are for extended clinic hours. The number of people opposed to spending anything for extended hours drops by nearly half, if the question is about after-hours acute care. Or, one could say that almost twice as many people are willing to see some tax dollars spent on after-hours Acute Care as there are wanting to spend it for extended hours.
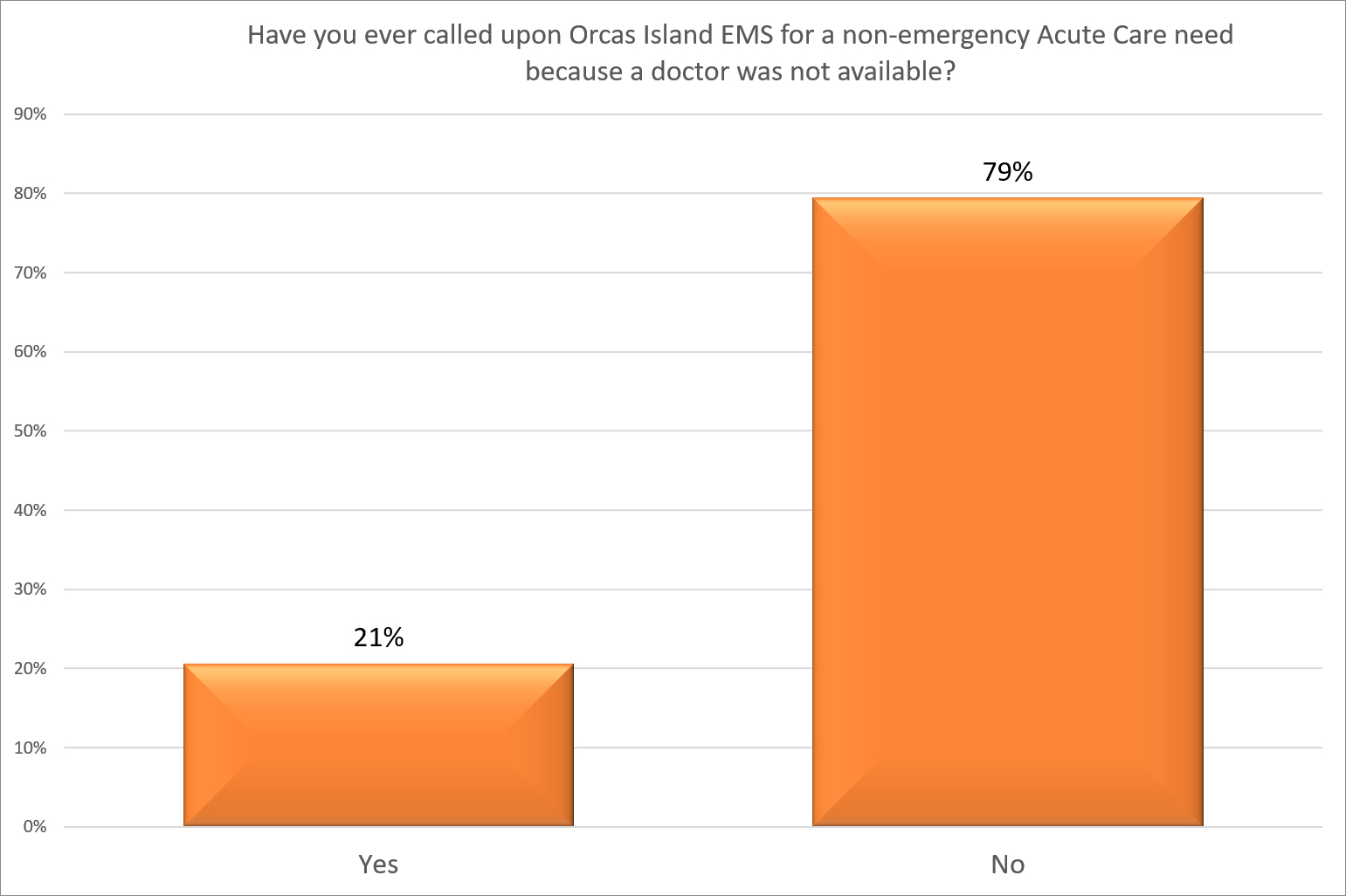
Q12 – Have you called on EMS due to a doctor not being available?
Q13 – Where do you currently receive your primary care?
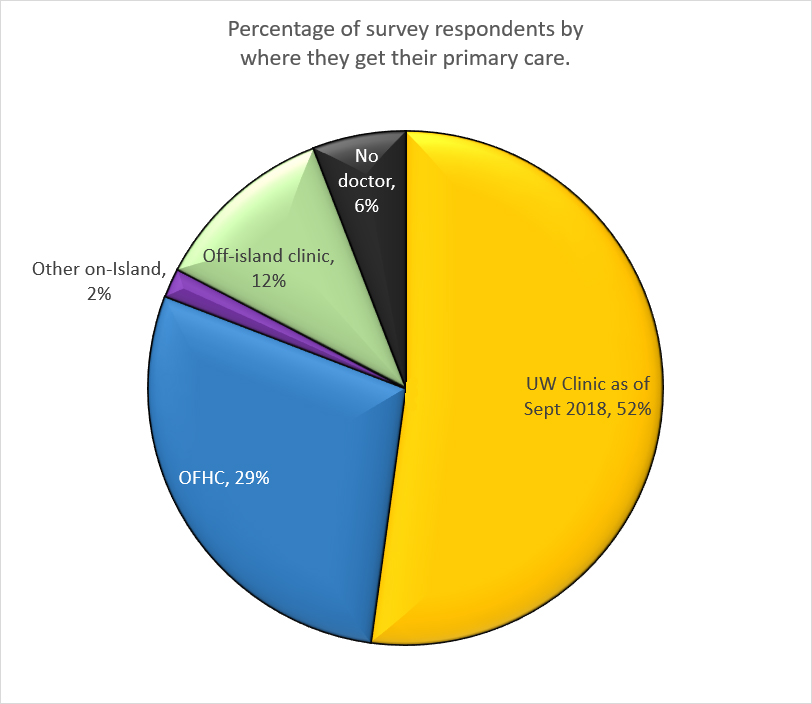
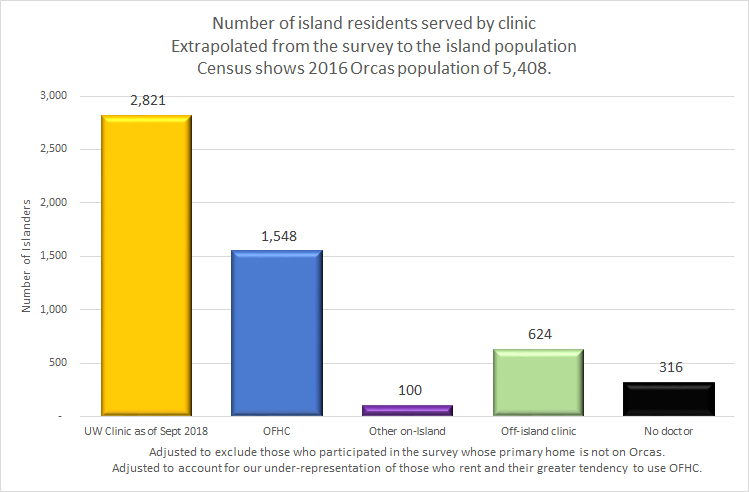
Percentages are adjusted to exclude those who took the survey but whose primary homes are not on the island. Percentages are also adjusted to account for our under-representation of those who rent and their greater tendency to visit OFHC.
Q13a – Population served by each clinic
Q14 And Q17 – Clinic satisfaction ratings
Based on the answer the respondent gave to question 13, which asked who a person’s primary care provider is, we directed them to a set of questions that are unique to their provider. In other words, those who use UW were asked to rate and comment on UW. Those who use OFHC were asked to rate and comment on OFHC. Those who use another island provider for their primary care were directed to a set of questions that asked who this provider is and then asked them to rate and comment on that provider. Those who use an off-island provider for their primary care were asked if their primary home is on Orcas and then why they don’t use island doctors for their primary care. At the end of the survey, there was a place for general comments, giving respondents the opportunity to share their thoughts on anything, including other providers other than their own.
The graphs on the following pages show the rating that respondents gave for the clinic or provider they identified as their primary care provider. The scale was 0 to 10. To calculate the average rating, we multiply the number of people giving the rating they chose and then sum the total of these multiplications. Then, we divide by the total number of respondents.
As we graph the information, we need to put the data for each clinic on the same vertical scale so the results are equally presented. This causes a lot of white space on one of the clinics, which is necessary for an unbiased comparison.
We summed the response for those giving a clinic a 7, 8, 9, or 10 and also summed those giving each clinic an 8, 9, or 10. We also summed the responses for those rating the clinics 0 to 4. Those are shown in the horizontal arrows.
We do not show a graph for those selecting “other island provider,” as there are insufficient responses for the numbers to be statistically valid.
Q13 OFHC rating
Comments about OFHC clinic
Appendix E – Comments about OFHC
The comments about the two clinics will help anyone wanting to better understand what is working well and what isn’t working well for primary medical care on Orcas Island. We publish the comments because we told you we would. There are many passionate comments, both expressing appreciation and frustration for the care and service they receive. As we mentioned in our statement above, health care matters to us all. In those rare instances where the comment was about the quality of the person(s) rather than the quality of the service given by the person(s) or it was constructive criticism but a name was mentioned in a manner that could create legal ramifications for someone, we either contacted the commenter to visit with them about it and they modified their own comment to be more helpful or we omitted their comment from public view but made sure the original (exactly as written) was shared with the commissioners and the clinic. Thank you for your understanding on that.
Q13 UW rating
Comments about the UW clinic
Appendix F – Comments about UW
The comments about the two clinics will help anyone wanting to better understand what is working well and what isn’t working well for primary medical care on Orcas Island. We publish the comments because we told you we would. There are many passionate comments, both expressing appreciation and frustration for the care and service they receive. As we mentioned in our statement above, health care matters to us all. In those rare instances where the comment was about the quality of the person(s) rather than the quality of the service given by the person(s) or it was constructive criticism but a name was mentioned in a manner that could create legal ramifications for someone, we either contacted the commenter to visit with them about it and they modified their own comment to be more helpful or we omitted their comment from public view but made sure the original (exactly as written) was shared with the commissioners and the clinic. Thank you for your understanding on that.
Q20-Q23 Other island providers
Five of our respondents identified Other island providers as their primary care provider. Each rated their provider highly.
| Provider | Comments | Liked about |
| Dr. Vincent Shu – rated 8 |
His facilities are limited, but his attention is marvelous | Personal relationship and availability |
| Dr Vincent Shu – rated 10 |
This physician us brilliant and is certified in cardiology, gerontology, and internal Medicine. My second choice is Dr. Russell the only one that my insurance will pay for because he is employed by UW. However, because I could not communicate with Dr. Russell, I contacted Dr Shu and he kept in close touch with me asking for my vitals frequently because he was concerned. He is the one who told me then to go to EMS or Friday Harbor and he probably would have taken me himself had he not been in Anacortes. Therefore, I felt strong enough to drive although I knew something was very wrong as did Dr. Shu. Rather than try to find someone to drive me, I decided to drive to Friday Harbor to Peace Health and my heart stopped shortly after I arrived while I was on the gurney. Had I been able to get an appointment when symptoms first appeared on a regular basis in mid- June, I could have avoided the dangerous situation I was in on June 27th. Other people in that same situation could have died because symptoms are not that noticeable to someone not having the medical education that I have had and had they no way to monitor their vitals. | His compassionate concern about his patients and his dedication to research and of course, his availability. Finally his brilliance. I am from a family of physicians so I recognize his brilliance. My deceased husband was like him in that respect. |
| Dr. Tina Torri ND, LAc rated 10 |
||
| Dr Kami Rathburn – rated 9 | She listens. She’s known me for 13 yrs will make referrals and cares. She’s intelligent about bodies. | |
| An unidentified acupuncturist and chiropractor- rated 8 |
Along with dental care, i have no coverage. Everything requires cash. Along with exercise classes, massage therapy | I leave a treatment feeling great…or so much better |
Q24 – Off-island provider
We asked those who identified their primary care provider as being off-island if their primary home is on Orcas Island.
Comments about why some do not doctor on island.
Demographic questions
We use these to help us test whether or not the survey is representative of the community and, if necessary, how to compensate for it. We also use demographic questions to see if there are differences in policy decision preferences based on various demographic characteristics.
Q26 – Gender
Q27 – Children under the age of 18?
Q28 – Age – Survey compared to Voters
Q28 – Age – Survey compared to Voters and Population
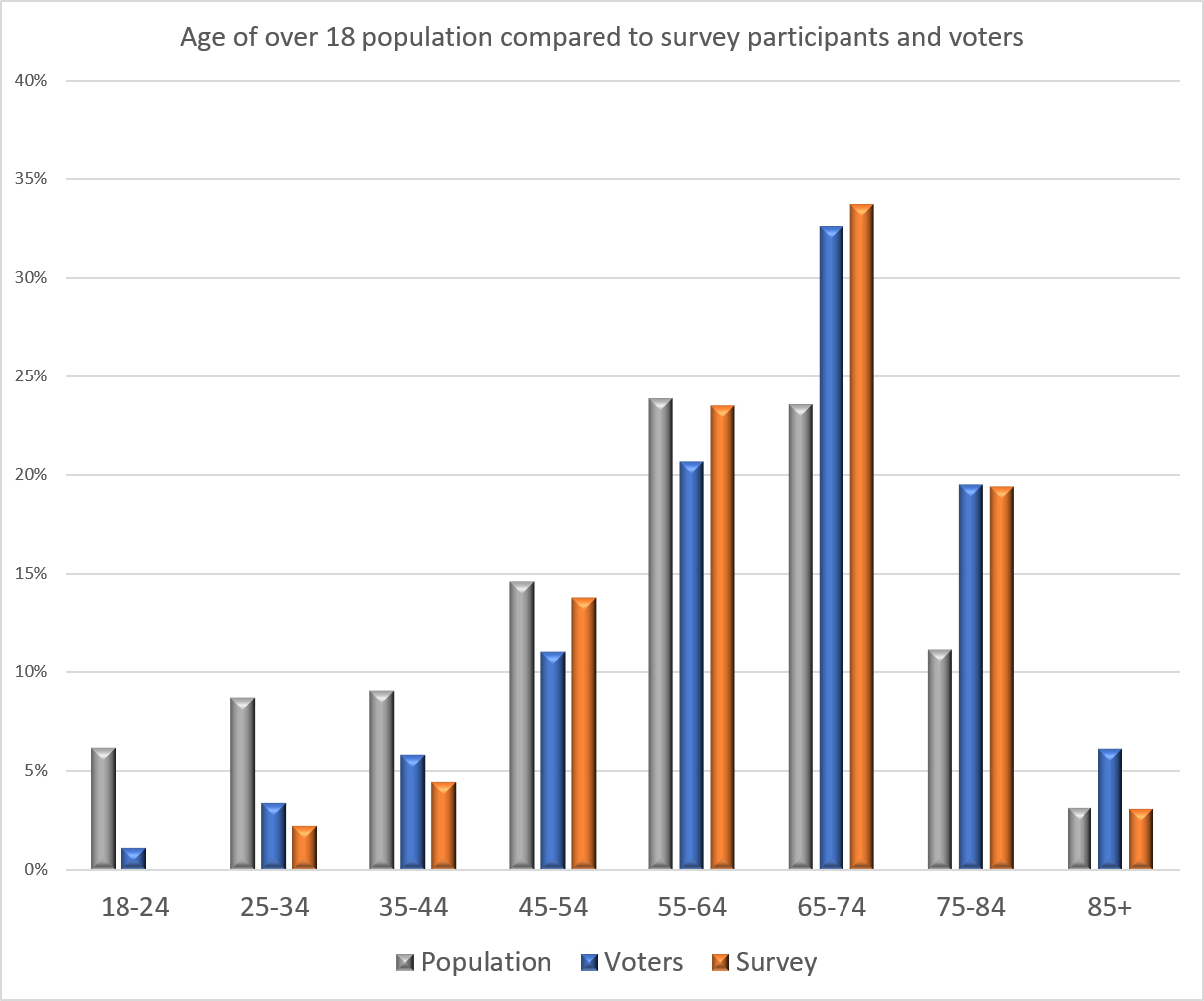
The blue bar is higher than the grey bar for those that are over 85 because of the ratios between various groups. See our study on the relationship of voting to age.
Q29 – Home Tenancy
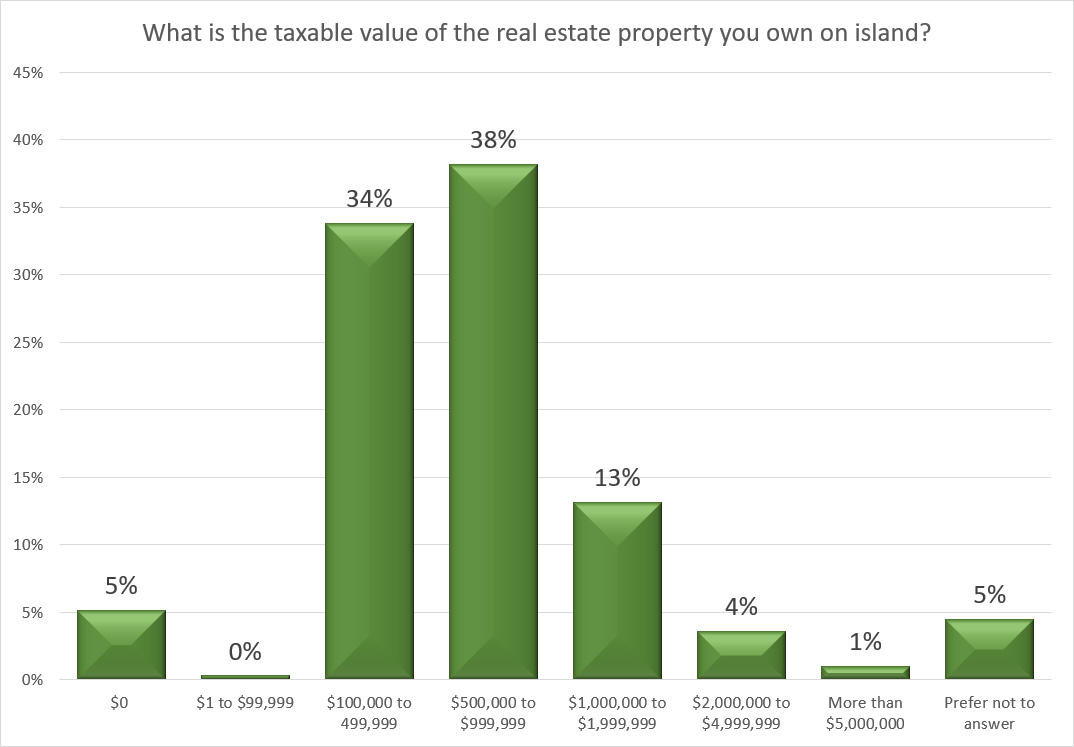
Q30 Property Values
Q31 – General Comments
We closed the survey by asking people to make any comment they liked.
Comparisons
Here, we summarize the survey results from the perspective of different demographic groups.
Based on Gender
- There are very few differences between the genders in regard to policy.
- Females are more likely to be renters than male.
- Females are more common in the no taxable property category.
Based on Home Tenancy
- Those who rent are more likely to have called on the EMS because a doctor was not available.
- Those who rent are much more likely to use OFHC for their primary care provider
- Those who own their home are much more likely to use UW clinic for their primary care.
- Those who rent tend to not have any taxable property
- About 20% of those who rent report taxable property worth $100k to $500k.
- The homeowners and the renters both have the same demands for time till an appointment.
- The homeowners and the renters both have very similar attitudes toward spending for extended hours and after-hours care.
Based on Property Value
- Those with no taxable property are more inclined to want to increase clinic access by adding hours, adding Saturday morning, and shifting clinic hours.
- All of those with no taxable property want everyone, regardless of residency, to have access to Acute Care. All other property groups have about 10% who want to restrict access based on residency.
- Those with no taxable property are much more likely (45%) to have called on the EMS for non-emergency Acute Care because a doctor was not available than those of other property status. Those with some taxable property average around 22% who have called on the EMS for this reason.
- Those with no taxable property are more likely to be patients of OFHC than any other property status group.
- Those with the most property value are much more likely to have their primary care provider off-island. However, the more valuable the property, the more likely their primary home is on-island.
- Those with no taxable property are much more likely to be female and to have children in the home.
- Those with more property valued between half million and two million are the least likely to have children at home.
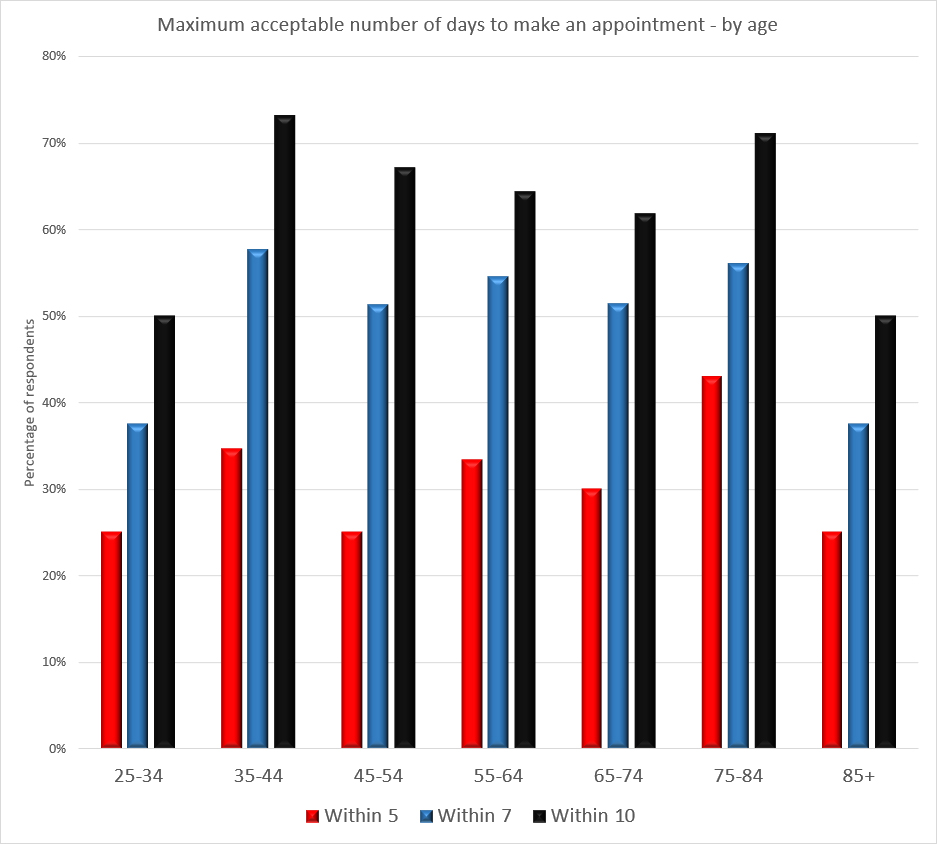
Based on Age
- The youngest are willing to wait the longest for appointments. The 75-84 age group is willing to wait the least amount of time, with 43% wanting to be able to make appointments within five days.
- There is little difference between the ages for the other responses.
This graph shows that 40% of those between the ages of 75 and 84 want appointments to be within 5 days of a call. We omit the days longer than 10 days till an appointment to make the graph easier to read. The youngest and oldest age groups are the most willing to wait.
All Comments in one place
-
Increasing Access Comments
-
Access to Acute Care DURING clinic hours Comments
-
Access to Acute Care AFTER clinic hours Comments
-
Comments about OFHC
-
Comments about UW
-
Comments from those who do not doctor on-island about why they don’t
-
General Comments
Is the survey representative of the community?
Please see Appendix A for a more detailed review.
Our comments about the survey
According to the 2016 Census estimates, the adult population of the island is 4,793. We have run four policy surveys this year, our first year. We have had approximately 1,100 unique people take our surveys. This survey saw about 180 new participants that had not participated in any of our earlier surveys.
As in previous surveys, we answered questions about accessing the survey and assisted people in accessing it when needed — in email, over the phone, and in person with provided equipment. We experienced problems with sending emails to mac.com and icloud.com email addresses with this survey. Thank you to Captain Rex for helping get this problem resolved. We were eventually able to send invitations to all email addresses on our list.
We extended the survey deadline by eleven days. We saw an additional 39 people take the survey in that time. Ten of those were people who had not already received an invitation. The additional time did not increase the accuracy of the survey nor affect any one data point by more than 1%.
We received 77% of our responses within the first two days. In the first week, we received 94% of the responses.
Terminology. We try to be straight-forward in our wording, but several topics entail terms that are specialized to that subject. Such is the case with health care. For example, “acute care,” “urgent care,” and “primary care.” At times, there is a difference in opinion on definitions, even among those who work in the field. It could be because of a difference in experiences or a difference in training. This can be an issue in surveys. In order to minimize confusion regarding what the survey writers mean in the text of the questions and available options to select, we have a number of people work on creating the language. Multiple people review the words that could be used and come to an agreement on particular word usage as well as how they are defined. Then, those definitions are placed in the survey.
Representing the community. We will continue to work on finding ways to encourage renters and those who are under the age of 35 to participate in greater numbers. We are not unique in having difficulty in obtaining participation from these groups. Some people just don’t participate, even though they are aware of the opportunity. Some people don’t participate because they don’t use the internet. Some are not currently interested. Some simply have not found out about us yet. We do try to encourage participation, and we are grateful to those of you helping to spread the word to others that this opportunity is available. Please see our website for much more information about what we are doing to reach groups not currently participating in surveys.
Thank you for trusting us and taking our surveys.
Madrona Voices